S-ar putea să vă placă și
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- An Open Letter To My Daughter: Rebecca L. FisherDocument2 paginiAn Open Letter To My Daughter: Rebecca L. Fisherrfisher284_164995324Încă nu există evaluări
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Final Programme A4 - IPOS 2023 - CompressedDocument60 paginiFinal Programme A4 - IPOS 2023 - CompressedFlorinaÎncă nu există evaluări
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- Dr. Lederman Responds To Questions From Dr. Kornhauser Regarding Body RadiosurgeryDocument6 paginiDr. Lederman Responds To Questions From Dr. Kornhauser Regarding Body RadiosurgeryGil LedermanÎncă nu există evaluări
- Iscador EBM91 PDFDocument208 paginiIscador EBM91 PDFJose CaceresÎncă nu există evaluări
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- Patients With Rectal Cancer: CopenhagenDocument5 paginiPatients With Rectal Cancer: CopenhagenAnonymous BHBsxWÎncă nu există evaluări
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- Pre-Invasive Lesions of The Cervix 2020Document58 paginiPre-Invasive Lesions of The Cervix 2020Jeno Luis J. ACUBÎncă nu există evaluări
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- ALGORITH Systemic Therapy For Advanced Hepatocellular Carcinoma AlgorithmDocument1 paginăALGORITH Systemic Therapy For Advanced Hepatocellular Carcinoma Algorithmhenok seifeÎncă nu există evaluări
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Case Presentation OralcavityDocument33 paginiCase Presentation Oralcavityapi-250609678Încă nu există evaluări
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- Breast Imaging Companion 2001 - CardenosaDocument509 paginiBreast Imaging Companion 2001 - CardenosaDanaÎncă nu există evaluări
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- PBL CASE 2 Module 13 Reproductive SystemDocument25 paginiPBL CASE 2 Module 13 Reproductive SystemkaraenÎncă nu există evaluări
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Oncology Nursing - OverviewDocument137 paginiOncology Nursing - OverviewMae DacerÎncă nu există evaluări
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- Neck DissectionDocument43 paginiNeck DissectionMeilina Elin WardhaniÎncă nu există evaluări
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- 005Document16 pagini005S PERSIS ALEXÎncă nu există evaluări
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- Assignment No 1 bt502 SeminarDocument15 paginiAssignment No 1 bt502 SeminarMashal WakeelaÎncă nu există evaluări
- Basal Cell Carcinoma - Pathophysiology and ManagementDocument6 paginiBasal Cell Carcinoma - Pathophysiology and ManagementReylan Garcia0% (1)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- FNA Biopsy Thyroid Nodules BrochureDocument2 paginiFNA Biopsy Thyroid Nodules BrochureAndreeaBraduÎncă nu există evaluări
- Gambaran Pengetahuan Wanita Usia Subur Tentang Manfaat Iva Test Fardila Elba, Imma Kristy NathaliaDocument8 paginiGambaran Pengetahuan Wanita Usia Subur Tentang Manfaat Iva Test Fardila Elba, Imma Kristy NathaliaYuni AnggrayniÎncă nu există evaluări
- Appendigeal TumoursDocument3 paginiAppendigeal TumourspritanuÎncă nu există evaluări
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (345)
- Actinic Keratosis: (Aka Bowen's Disease)Document5 paginiActinic Keratosis: (Aka Bowen's Disease)fadoÎncă nu există evaluări
- Susan G Komen EssayDocument6 paginiSusan G Komen Essayapi-248182825Încă nu există evaluări
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- Breast Pathology Group 1Document67 paginiBreast Pathology Group 1chacha 7074684Încă nu există evaluări
- Update To The College of American Pathologists Reporting On Thyroid CarcinomasDocument8 paginiUpdate To The College of American Pathologists Reporting On Thyroid CarcinomasMuhammad FiqranÎncă nu există evaluări
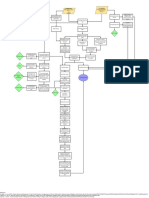
- Kaposi-Sarcoma PathophysiologyDocument1 paginăKaposi-Sarcoma PathophysiologyChiara FajardoÎncă nu există evaluări
- BAHNO 2016 GuidelinesDocument52 paginiBAHNO 2016 GuidelinesNooeÎncă nu există evaluări
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- Introduction To Oncology NursingDocument35 paginiIntroduction To Oncology NursingDesh Deepak100% (1)
- Oral Cavity CancerDocument16 paginiOral Cavity CancerIlma Kurnia SariÎncă nu există evaluări
- Intraoperative CytologyDocument86 paginiIntraoperative Cytologypreeti sharmaÎncă nu există evaluări
- Case Study #5Document2 paginiCase Study #5Jenny Jenders100% (1)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Lesson Plan SynopsisDocument19 paginiLesson Plan Synopsisshivani dasÎncă nu există evaluări
- Kaposi's Sarcoma: Patients Seen in The Past 8 Years: 83 CasesDocument12 paginiKaposi's Sarcoma: Patients Seen in The Past 8 Years: 83 CasesWorku KifleÎncă nu există evaluări
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)