S-ar putea să vă placă și
- Complementary and Alternative Medical Lab Testing Part 1: EENT (Eyes, Ears, Nose and Throat)De la EverandComplementary and Alternative Medical Lab Testing Part 1: EENT (Eyes, Ears, Nose and Throat)Încă nu există evaluări
- Case-Control Study of Body Size and Breast Cancer Risk in Nigerian WomenDocument9 paginiCase-Control Study of Body Size and Breast Cancer Risk in Nigerian WomenGEDE PRONAJAYAÎncă nu există evaluări
- Week 8 Data Interpretation Epidoria Birth Study Online KEYDocument2 paginiWeek 8 Data Interpretation Epidoria Birth Study Online KEYJoshMatthewsÎncă nu există evaluări
- Determinant Factors of Stunting Events of Toddler in Batu City IndonesiaDocument4 paginiDeterminant Factors of Stunting Events of Toddler in Batu City IndonesiaAlfian B. PrasetyoÎncă nu există evaluări
- Issu PNC IndiaDocument4 paginiIssu PNC IndiaInezya AyuditaÎncă nu există evaluări
- Rahayu & Wahyu, 2021Document8 paginiRahayu & Wahyu, 2021Chingura LuffyÎncă nu există evaluări
- Review Questions-Association and BiasDocument12 paginiReview Questions-Association and BiassanjivdasÎncă nu există evaluări
- Pediatric NursingDocument6 paginiPediatric NursingAllisson BeckersÎncă nu există evaluări
- 2. Evaluation - ANSWERSDocument15 pagini2. Evaluation - ANSWERSrobinsonbryÎncă nu există evaluări
- Short Stature in Childhood - Challenges and ChoicesDocument9 paginiShort Stature in Childhood - Challenges and ChoicesEsteban Martin Chiotti KaneshimaÎncă nu există evaluări
- Anemia in Pre-School Children-Does Time Change Anything?Document5 paginiAnemia in Pre-School Children-Does Time Change Anything?NZ FreelancersÎncă nu există evaluări
- Linear Growth and Neurodevelopmental Outcome of Children With Congenital Hypothyroidism Detected by Neonatal Screening: A Controlled StudyDocument4 paginiLinear Growth and Neurodevelopmental Outcome of Children With Congenital Hypothyroidism Detected by Neonatal Screening: A Controlled StudyajaysardesaiÎncă nu există evaluări
- Listen: Blood CultureDocument4 paginiListen: Blood CultureVasundhara MeghaÎncă nu există evaluări
- Growth and Development in PediatricsDocument67 paginiGrowth and Development in PediatricsMahmoud SuleimanÎncă nu există evaluări
- Peads OsceDocument6 paginiPeads OsceFarazÎncă nu există evaluări
- Biological Variations Technical StabilitDocument8 paginiBiological Variations Technical StabilitOumar SourabieÎncă nu există evaluări
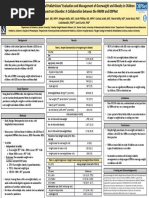
- Developmental-Behavioral Pediatricians' Evaluation and Management of Overweight and Obesity in Children With ASD: A Collaboration Between The HWRN and DBPNet (Sarabeth Broder-Fingert)Document1 paginăDevelopmental-Behavioral Pediatricians' Evaluation and Management of Overweight and Obesity in Children With ASD: A Collaboration Between The HWRN and DBPNet (Sarabeth Broder-Fingert)AUCDÎncă nu există evaluări
- Pharmaceutical Sciences: Congenital Hypothyroidism Prevalence Diagnosis and Outcome in Saudi ArabiaDocument5 paginiPharmaceutical Sciences: Congenital Hypothyroidism Prevalence Diagnosis and Outcome in Saudi ArabiaiajpsÎncă nu există evaluări
- Associations Between Red Blood Cell and Platelet Transfusions and Retinopathy of PrematurityDocument7 paginiAssociations Between Red Blood Cell and Platelet Transfusions and Retinopathy of PrematurityclaudyÎncă nu există evaluări
- Clinical Guide To Transfusion - Neonatal and Pediatric Transfusion (Chapter 13)Document11 paginiClinical Guide To Transfusion - Neonatal and Pediatric Transfusion (Chapter 13)Mudzakir TaufiqÎncă nu există evaluări
- Fix Jurnal InterDocument6 paginiFix Jurnal InterFildzah DheaÎncă nu există evaluări
- IBÁÑEZ Et Al., 2011Document4 paginiIBÁÑEZ Et Al., 2011Luana BarrosÎncă nu există evaluări
- Lecture 2 - Assessment of Growth and It's Abnormality, Dr.S.yudha Patria, Sp.a (K) ., PH.D (2021)Document58 paginiLecture 2 - Assessment of Growth and It's Abnormality, Dr.S.yudha Patria, Sp.a (K) ., PH.D (2021)Dzaki Prakoso RamadhanÎncă nu există evaluări
- Evaluation of Blood Pressure in Children With Hydronephrosis in Comparison With Healthy ChildrenDocument3 paginiEvaluation of Blood Pressure in Children With Hydronephrosis in Comparison With Healthy ChildrenLuyến Nguyễn NhưÎncă nu există evaluări
- Prenatal Vitamin D Status and Offsprings Growth Adiposity and Metabolic Health A Systematic Review and Meta AnalysisDocument10 paginiPrenatal Vitamin D Status and Offsprings Growth Adiposity and Metabolic Health A Systematic Review and Meta Analysismisslcassidy2Încă nu există evaluări
- Normal HB in Children - Google SearchDocument1 paginăNormal HB in Children - Google SearchKasuba KapayaÎncă nu există evaluări
- Dyslipidemia in Children and Adolescents: When and How To Diagnose and Treat?Document8 paginiDyslipidemia in Children and Adolescents: When and How To Diagnose and Treat?leslyjanetÎncă nu există evaluări
- Socio-Demographics Aspects and Adolescent's ObesityDocument7 paginiSocio-Demographics Aspects and Adolescent's ObesityShilpa KhotÎncă nu există evaluări
- Waist Circumference, Waist-to-Height Ratio, and Waist-to-Hip Ratio Profiles of Under-Fives Children From A Cohort Study in BogorDocument9 paginiWaist Circumference, Waist-to-Height Ratio, and Waist-to-Hip Ratio Profiles of Under-Fives Children From A Cohort Study in BogorMURSID TRI SUSILOÎncă nu există evaluări
- Metabolic Syndrome in Very Low Birth Weight Young Adults and Controls: The New Zealand 1986 VLBW StudyDocument11 paginiMetabolic Syndrome in Very Low Birth Weight Young Adults and Controls: The New Zealand 1986 VLBW StudysatishÎncă nu există evaluări
- Background: CKD of Uncertain Etiology Sri Lanka A Population Study at Girandurukotte, Uva Province, Preliminary ReportDocument6 paginiBackground: CKD of Uncertain Etiology Sri Lanka A Population Study at Girandurukotte, Uva Province, Preliminary Reportsumanenthiran123Încă nu există evaluări
- Dietary Fat and AMD RiskDocument16 paginiDietary Fat and AMD RiskAngellaÎncă nu există evaluări
- Predicting Early Childhood ObesityDocument6 paginiPredicting Early Childhood ObesityNancy Dalla DarsonoÎncă nu există evaluări
- Leschek 2004Document9 paginiLeschek 2004GutoGonçalvesÎncă nu există evaluări
- Examination of Young Children With Lea SymbolsDocument6 paginiExamination of Young Children With Lea SymbolsArturo GuilliemÎncă nu există evaluări
- Knowledge Attitudes and Practices Regarding Diabetes Mellitus Among University Students in Jeddah Saudi ArabiaDocument9 paginiKnowledge Attitudes and Practices Regarding Diabetes Mellitus Among University Students in Jeddah Saudi ArabiaCharles BagendaÎncă nu există evaluări
- Helen Bardsley Austin Health NICE 2012Document17 paginiHelen Bardsley Austin Health NICE 2012Akrm Al-komimÎncă nu există evaluări
- Genetic Testing Explained: Benefits, Risks and Future PossibilitiesDocument3 paginiGenetic Testing Explained: Benefits, Risks and Future PossibilitiesPili116Încă nu există evaluări
- Fped 09 801955Document9 paginiFped 09 801955YandiÎncă nu există evaluări
- Lipid Profile in ChildrenDocument8 paginiLipid Profile in Childrenheema valeraÎncă nu există evaluări
- Idiopathic Short Stature Definition EpidDocument9 paginiIdiopathic Short Stature Definition Epidfrancisco perezÎncă nu există evaluări
- 10 1056@NEJMoa1905593Document11 pagini10 1056@NEJMoa1905593Eghar EverydayishellÎncă nu există evaluări
- NUTRITIONAL AssessmentDocument46 paginiNUTRITIONAL AssessmentSonali Hazra0% (1)
- 1 s2.0 S1658361219301052 MainDocument9 pagini1 s2.0 S1658361219301052 MainkalwusaidiÎncă nu există evaluări
- 27 GiuliodoriMJJDS96 3621 Metritisindairycows 2013Document21 pagini27 GiuliodoriMJJDS96 3621 Metritisindairycows 2013awaluzzikryÎncă nu există evaluări
- Breast vs. Bottle: Differences in The Growth of Croatian InfantsDocument9 paginiBreast vs. Bottle: Differences in The Growth of Croatian InfantsBernadette Grace RetubadoÎncă nu există evaluări
- Pediatrics Revision E6.5 @TheBoggusdocDocument55 paginiPediatrics Revision E6.5 @TheBoggusdocsushmaÎncă nu există evaluări
- Childhood Obesity Linked to Accelerated Dental DevelopmentDocument5 paginiChildhood Obesity Linked to Accelerated Dental DevelopmentRoxana OneaÎncă nu există evaluări
- Pediatric Lead Exposure Flint Water ResultsDocument20 paginiPediatric Lead Exposure Flint Water ResultsDetroit Free PressÎncă nu există evaluări
- Jurnal HemaDocument38 paginiJurnal HemaJohan GautamaÎncă nu există evaluări
- Article Pour TraductionDocument5 paginiArticle Pour TraductionMa NelÎncă nu există evaluări
- Designer Babies22Document2 paginiDesigner Babies22Adi DianÎncă nu există evaluări
- Dwarfism Term PaperDocument6 paginiDwarfism Term Paperaflrpjser100% (1)
- SJAMS 611 4541 4545 CDocument5 paginiSJAMS 611 4541 4545 CMeiyanti MeiyantiÎncă nu există evaluări
- 41.balaprasad Baheti Deepak Joshi Gorte Ranjeet Vidyasager Gali Nandkishor Bavge Shyamlila BavgeDocument18 pagini41.balaprasad Baheti Deepak Joshi Gorte Ranjeet Vidyasager Gali Nandkishor Bavge Shyamlila BavgeBalaprasad BahetiÎncă nu există evaluări
- RDA PediatricsDocument49 paginiRDA PediatricsAnugrah NoviantiÎncă nu există evaluări
- Review of Catch-Up Growth in Full-Term SGA InfantsDocument8 paginiReview of Catch-Up Growth in Full-Term SGA InfantsAdib FraÎncă nu există evaluări
- Childhood Obesity in Iraq: Prevalence and Possible Risk FactorsDocument5 paginiChildhood Obesity in Iraq: Prevalence and Possible Risk FactorsAli AlhamdaniÎncă nu există evaluări
- Environmental Research: SciencedirectDocument13 paginiEnvironmental Research: SciencedirectSunita ChayalÎncă nu există evaluări
- The Risk Level For Individuals To Suffering From NCDs Based On CERDIK BehaviorDocument6 paginiThe Risk Level For Individuals To Suffering From NCDs Based On CERDIK BehaviorIJPHSÎncă nu există evaluări
- Meal 1: Add Food Quick ToolsDocument2 paginiMeal 1: Add Food Quick ToolsJoshMatthewsÎncă nu există evaluări
- Session RecapsDocument2 paginiSession RecapsJoshMatthewsÎncă nu există evaluări
- The Resurgence of Infectious DiseasesDocument19 paginiThe Resurgence of Infectious DiseasesJoshMatthewsÎncă nu există evaluări
- Capital University public health major course requirements overviewDocument4 paginiCapital University public health major course requirements overviewJoshMatthewsÎncă nu există evaluări
- Soc 360-01-Social Problems CeDocument10 paginiSoc 360-01-Social Problems CeJoshMatthewsÎncă nu există evaluări
- Marvel QuizDocument5 paginiMarvel QuizJoshMatthewsÎncă nu există evaluări
- Outbreak Investigations: The 10-Step ApproachDocument40 paginiOutbreak Investigations: The 10-Step ApproachJoshMatthewsÎncă nu există evaluări
- Session RecapsDocument2 paginiSession RecapsJoshMatthewsÎncă nu există evaluări
- EditorialDocument6 paginiEditorialJoshMatthewsÎncă nu există evaluări
- The Biomedical Basis of Chronic DiseasesDocument17 paginiThe Biomedical Basis of Chronic DiseasesJoshMatthewsÎncă nu există evaluări
- Syllabus Boilerplate UpdatedDocument3 paginiSyllabus Boilerplate UpdatedJoshMatthewsÎncă nu există evaluări
- The "Conquest" of Infectious DiseasesDocument15 paginiThe "Conquest" of Infectious DiseasesJoshMatthewsÎncă nu există evaluări
- Public Health Major RequirementsDocument1 paginăPublic Health Major RequirementsJoshMatthewsÎncă nu există evaluări
- Capital PH Major Design Ea. Total Milage: 2 66 Mi. (1 Trip) Time: 3 Meetings: 1Document1 paginăCapital PH Major Design Ea. Total Milage: 2 66 Mi. (1 Trip) Time: 3 Meetings: 1JoshMatthewsÎncă nu există evaluări
- Personal Training Agreement Form and Cancellation PolicyDocument1 paginăPersonal Training Agreement Form and Cancellation PolicyJoshMatthewsÎncă nu există evaluări
- Conditioning and Strength Program ARMYPTDocument1 paginăConditioning and Strength Program ARMYPTJoshMatthewsÎncă nu există evaluări
- Discover the Mysteries of the Echo WoodDocument30 paginiDiscover the Mysteries of the Echo WoodJoshMatthewsÎncă nu există evaluări
- Public Health Mission and Learning OutcomesDocument1 paginăPublic Health Mission and Learning OutcomesJoshMatthewsÎncă nu există evaluări
- 4-Day Full Body Strength Workout with Weekly ProgressionDocument7 pagini4-Day Full Body Strength Workout with Weekly ProgressionJoshMatthewsÎncă nu există evaluări
- Temple of SandpointDocument1 paginăTemple of SandpointJoshMatthewsÎncă nu există evaluări
- Early Alert-V2 - Research Forester (2 (Document3 paginiEarly Alert-V2 - Research Forester (2 (JoshMatthewsÎncă nu există evaluări
- Discover the Mysteries of the Echo WoodDocument30 paginiDiscover the Mysteries of the Echo WoodJoshMatthewsÎncă nu există evaluări
- Employee attendance records Jan 2022Document1 paginăEmployee attendance records Jan 2022JoshMatthewsÎncă nu există evaluări
- D&D item compendium under 40 charsDocument4 paginiD&D item compendium under 40 charsYukonCorneliousÎncă nu există evaluări
- The Spire of The Hunting Sound-Characters and Mini Bestiary-2017!06!02Document17 paginiThe Spire of The Hunting Sound-Characters and Mini Bestiary-2017!06!02Faz Maldov100% (2)
- The Program: Day 1 - Full Body PushDocument4 paginiThe Program: Day 1 - Full Body PushJoshMatthewsÎncă nu există evaluări
- Discover the Mysteries of the Echo WoodDocument30 paginiDiscover the Mysteries of the Echo WoodJoshMatthewsÎncă nu există evaluări
- Undergraduate Public Health SyllabusDocument5 paginiUndergraduate Public Health SyllabusJoshMatthewsÎncă nu există evaluări
- Updated Babysitting TestDocument6 paginiUpdated Babysitting TestJoshMatthewsÎncă nu există evaluări
- Babysitters Training Instructor Bulletin May 2016 v4Document3 paginiBabysitters Training Instructor Bulletin May 2016 v4gadissagitaÎncă nu există evaluări
- SQL 1: Basic Statements: Yufei TaoDocument24 paginiSQL 1: Basic Statements: Yufei TaoHui Ka HoÎncă nu există evaluări
- EQ - Module - Cantilever MethodDocument17 paginiEQ - Module - Cantilever MethodAndrea MalateÎncă nu există evaluări
- Mythic Magazine 017Document43 paginiMythic Magazine 017William Warren100% (1)
- C11 RacloprideDocument5 paginiC11 RacloprideAvina 123Încă nu există evaluări
- The Emperor Jones: What's Inside in ContextDocument27 paginiThe Emperor Jones: What's Inside in ContextHarshvardhan RaiÎncă nu există evaluări
- Hotel Design Planning and DevelopmentDocument30 paginiHotel Design Planning and DevelopmentTio Yogatma Yudha14% (7)
- Korba - BAH Online Temp MonitoringDocument7 paginiKorba - BAH Online Temp Monitoringrama jenaÎncă nu există evaluări
- The Graduation Commencement Speech You Will Never HearDocument4 paginiThe Graduation Commencement Speech You Will Never HearBernie Lutchman Jr.Încă nu există evaluări
- 01 Design of Flexible Pavement Using Coir GeotextilesDocument126 pagini01 Design of Flexible Pavement Using Coir GeotextilesSreeja Sadanandan100% (1)
- 67c Series Bulletin 08 04 PDFDocument12 pagini67c Series Bulletin 08 04 PDFnight wolfÎncă nu există evaluări
- StsDocument10 paginiStsSamonte, KimÎncă nu există evaluări
- HP OpenVMS Alpha Version 8.3 and HP OpenVMS Version 8.3-1H1 For IntegrityDocument65 paginiHP OpenVMS Alpha Version 8.3 and HP OpenVMS Version 8.3-1H1 For IntegrityAlexandru BotnariÎncă nu există evaluări
- Relay Coordination Using Digsilent PowerFactoryDocument12 paginiRelay Coordination Using Digsilent PowerFactoryutshab.ghosh2023Încă nu există evaluări
- Analysis of VariancesDocument40 paginiAnalysis of VariancesSameer MalhotraÎncă nu există evaluări
- Java MCQ QuestionsDocument11 paginiJava MCQ QuestionsPineappleÎncă nu există evaluări
- Merchandise Floor Ready Standards - Supplier InformationDocument46 paginiMerchandise Floor Ready Standards - Supplier InformationGarmentLearner100% (1)
- 256267a1Document5.083 pagini256267a1Елизавета ШепелеваÎncă nu există evaluări
- Flexible AC Transmission SystemsDocument51 paginiFlexible AC Transmission SystemsPriyanka VedulaÎncă nu există evaluări
- LLoyd's Register Marine - Global Marine Safety TrendsDocument23 paginiLLoyd's Register Marine - Global Marine Safety Trendssuvabrata_das01100% (1)
- Raychem Price ListDocument48 paginiRaychem Price ListramshivvermaÎncă nu există evaluări
- Storytelling ScriptDocument2 paginiStorytelling ScriptAnjalai Ganasan100% (1)
- Ch. 7 - Audit Reports CA Study NotesDocument3 paginiCh. 7 - Audit Reports CA Study NotesUnpredictable TalentÎncă nu există evaluări
- The Rich Hues of Purple Murex DyeDocument44 paginiThe Rich Hues of Purple Murex DyeYiğit KılıçÎncă nu există evaluări
- Nqs PLP E-Newsletter No68Document5 paginiNqs PLP E-Newsletter No68api-243291083Încă nu există evaluări
- Brooks Cole Empowerment Series Becoming An Effective Policy Advocate 7Th Edition Jansson Solutions Manual Full Chapter PDFDocument36 paginiBrooks Cole Empowerment Series Becoming An Effective Policy Advocate 7Th Edition Jansson Solutions Manual Full Chapter PDFlois.guzman538100% (12)
- SuffrageDocument21 paginiSuffragejecelyn mae BaluroÎncă nu există evaluări
- Hencher - Interpretation of Direct Shear Tests On Rock JointsDocument8 paginiHencher - Interpretation of Direct Shear Tests On Rock JointsMark2123100% (1)
- Quality CircleDocument33 paginiQuality CircleSudeesh SudevanÎncă nu există evaluări
- Migration (LIN 19/051: Specification of Occupations and Assessing Authorities) Instrument 2019Document28 paginiMigration (LIN 19/051: Specification of Occupations and Assessing Authorities) Instrument 2019Ajay palÎncă nu există evaluări
- Manual Bombas CHWDocument16 paginiManual Bombas CHWFred GarciaÎncă nu există evaluări
- A-level Biology Revision: Cheeky Revision ShortcutsDe la EverandA-level Biology Revision: Cheeky Revision ShortcutsEvaluare: 5 din 5 stele5/5 (5)
- How to Teach Nature Journaling: Curiosity, Wonder, AttentionDe la EverandHow to Teach Nature Journaling: Curiosity, Wonder, AttentionEvaluare: 4.5 din 5 stele4.5/5 (3)
- A-Level Chemistry Revision: Cheeky Revision ShortcutsDe la EverandA-Level Chemistry Revision: Cheeky Revision ShortcutsEvaluare: 4 din 5 stele4/5 (5)
- Simple STEAM: 50+ Science Technology Engineering Art and Math Activities for Ages 3 to 6De la EverandSimple STEAM: 50+ Science Technology Engineering Art and Math Activities for Ages 3 to 6Încă nu există evaluări
- Making and Tinkering With STEM: Solving Design Challenges With Young ChildrenDe la EverandMaking and Tinkering With STEM: Solving Design Challenges With Young ChildrenÎncă nu există evaluări
- Lower Secondary Science Workbook: Stage 8De la EverandLower Secondary Science Workbook: Stage 8Evaluare: 5 din 5 stele5/5 (1)
- Quantum Physics for Beginners: Simple Illustrated Guide to Discover with Practical Explanations the Paradoxes of the Life and Universe Reconsidering RealityDe la EverandQuantum Physics for Beginners: Simple Illustrated Guide to Discover with Practical Explanations the Paradoxes of the Life and Universe Reconsidering RealityEvaluare: 2 din 5 stele2/5 (1)
- On Teaching Science: Principles and Strategies That Every Educator Should KnowDe la EverandOn Teaching Science: Principles and Strategies That Every Educator Should KnowEvaluare: 4 din 5 stele4/5 (2)
- How to Think Like a Lawyer--and Why: A Common-Sense Guide to Everyday DilemmasDe la EverandHow to Think Like a Lawyer--and Why: A Common-Sense Guide to Everyday DilemmasEvaluare: 3 din 5 stele3/5 (1)
- An Introduction to the Periodic Table of Elements : Chemistry Textbook Grade 8 | Children's Chemistry BooksDe la EverandAn Introduction to the Periodic Table of Elements : Chemistry Textbook Grade 8 | Children's Chemistry BooksEvaluare: 5 din 5 stele5/5 (1)
- Stay Curious and Keep Exploring: 50 Amazing, Bubbly, and Creative Science Experiments to Do with the Whole FamilyDe la EverandStay Curious and Keep Exploring: 50 Amazing, Bubbly, and Creative Science Experiments to Do with the Whole FamilyÎncă nu există evaluări
- GCSE Biology Revision: Cheeky Revision ShortcutsDe la EverandGCSE Biology Revision: Cheeky Revision ShortcutsEvaluare: 4.5 din 5 stele4.5/5 (2)
- The Sky Above and the Mud Below: Lessons from Nature Preschools and Forest KindergartensDe la EverandThe Sky Above and the Mud Below: Lessons from Nature Preschools and Forest KindergartensÎncă nu există evaluări
- Science Action Labs Science Fun: Activities to Encourage Students to Think and Solve ProblemsDe la EverandScience Action Labs Science Fun: Activities to Encourage Students to Think and Solve ProblemsÎncă nu există evaluări
- Creative Investigations in Early Engineering and TechnologyDe la EverandCreative Investigations in Early Engineering and TechnologyÎncă nu există evaluări
- Cool Science Experiments for Kids | Science and Nature for KidsDe la EverandCool Science Experiments for Kids | Science and Nature for KidsÎncă nu există evaluări
- Google Sheets For Beginners: The Ultimate Step-By-Step Guide To Mastering Google Sheets To Simplify Data Analysis, Use Spreadsheets, Create Diagrams, And Boost ProductivityDe la EverandGoogle Sheets For Beginners: The Ultimate Step-By-Step Guide To Mastering Google Sheets To Simplify Data Analysis, Use Spreadsheets, Create Diagrams, And Boost ProductivityÎncă nu există evaluări