S-ar putea să vă placă și
- Critical Care Adult Insulin InfusionDocument2 paginiCritical Care Adult Insulin InfusionTunas AndriantoÎncă nu există evaluări
- Management of Anesthesia: Diabetes MellitusDocument29 paginiManagement of Anesthesia: Diabetes MellitusHari PrasadÎncă nu există evaluări
- Protocol For Intensive Intravenous Insulin Infusion For ICUDocument2 paginiProtocol For Intensive Intravenous Insulin Infusion For ICUburlacuraduuÎncă nu există evaluări
- Insulin Protocols J Krinsley Rev July 2011Document1 paginăInsulin Protocols J Krinsley Rev July 2011Nuha AL-YousfiÎncă nu există evaluări
- Yale IIP MICU120-160 2011Document2 paginiYale IIP MICU120-160 2011afm26Încă nu există evaluări
- Idiot NotesDocument53 paginiIdiot NotesRay PerezÎncă nu există evaluări
- IV Insulin Infusion Protocol TexasDocument2 paginiIV Insulin Infusion Protocol TexasJohb CaballeroÎncă nu există evaluări
- Target Range For Glycemic Control: 80-140 MG/DL (Generally 110 MG/DL)Document3 paginiTarget Range For Glycemic Control: 80-140 MG/DL (Generally 110 MG/DL)Otchi Pudtrie Wijaya100% (1)
- Insulin Sliding Scale Protocol For Type II Diabetic PatientsDocument3 paginiInsulin Sliding Scale Protocol For Type II Diabetic PatientsDaulat JosuaÎncă nu există evaluări
- JBDS 02 Nursing Management For DKA v1 20122022Document10 paginiJBDS 02 Nursing Management For DKA v1 20122022olazbt2000Încă nu există evaluări
- Managing Hyperglycemia in the ER and ICUDocument11 paginiManaging Hyperglycemia in the ER and ICUerikaÎncă nu există evaluări
- Pet HealthDocument5 paginiPet HealthMuhammad Hamza AlviÎncă nu există evaluări
- DiabetesDocument7 paginiDiabetesapi-142637023Încă nu există evaluări
- Endocrine System: Capillary Glucose MonitoringDocument34 paginiEndocrine System: Capillary Glucose Monitoringjoel david knda mj100% (1)
- Outdoor & Indoor Treatment of Diabetes MellitusDocument8 paginiOutdoor & Indoor Treatment of Diabetes MellitusDR. PRITHWIRAJ MAITIÎncă nu există evaluări
- Endocrinology Lab: Dr. Amani FilimbanDocument6 paginiEndocrinology Lab: Dr. Amani Filimbanziyad khalidÎncă nu există evaluări
- Sample Only - Not For Clinical UseDocument6 paginiSample Only - Not For Clinical Usenostra83Încă nu există evaluări
- Yale Insulin Drip Protocol (Target 100 139) PDFDocument2 paginiYale Insulin Drip Protocol (Target 100 139) PDFAprilia Christi SiwiÎncă nu există evaluări
- Oral glucose tolerance test (OGTT) ABDULAZIZ22009.10.19 فDocument30 paginiOral glucose tolerance test (OGTT) ABDULAZIZ22009.10.19 فaziz faydi100% (1)
- Teaching DemoDocument16 paginiTeaching DemoKenj Yolleth IbañezÎncă nu există evaluări
- Insulin Sliding ScaleDocument2 paginiInsulin Sliding Scaleberman fernandoÎncă nu există evaluări
- Quick NOteDocument7 paginiQuick NOteAuni Akif Aleesa100% (1)
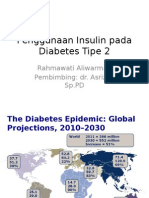
- Penggunaan Insulin Pada Diabetes Tipe 2Document47 paginiPenggunaan Insulin Pada Diabetes Tipe 2Dinny Novia WÎncă nu există evaluări
- Sick Day Rules New GuidelineDocument4 paginiSick Day Rules New Guidelinerahmatullahmandozai789Încă nu există evaluări
- Inpatient Guideline JoslinDocument8 paginiInpatient Guideline Joslinospinu6780Încă nu există evaluări
- 2017 05 GC Pocket CardDocument2 pagini2017 05 GC Pocket Cardapi-312241089Încă nu există evaluări
- Glycemic Management Guideline: General PrinciplesDocument8 paginiGlycemic Management Guideline: General PrinciplesJon KnezevichÎncă nu există evaluări
- Glucose Tolerance TestDocument21 paginiGlucose Tolerance TestRahma AbdullahÎncă nu există evaluări
- B. Other Possible Test B.1 Glucose-Fasting Blood Sugar (FBS) (Blood)Document3 paginiB. Other Possible Test B.1 Glucose-Fasting Blood Sugar (FBS) (Blood)elvie21Încă nu există evaluări
- Management of Diabetic Cats With Long Acting InsulinDocument16 paginiManagement of Diabetic Cats With Long Acting Insulindia_dianneÎncă nu există evaluări
- Insulin Initiation PPT - PPTX 2Document53 paginiInsulin Initiation PPT - PPTX 2Meno Ali100% (1)
- Blood Glucose Oki Aziz894180Document77 paginiBlood Glucose Oki Aziz894180aziz faydiÎncă nu există evaluări
- Vital Signs ReferenceDocument177 paginiVital Signs ReferenceQueenie FarrahÎncă nu există evaluări
- DkaDocument83 paginiDkaRajaKumar Ponnana100% (1)
- Glycemic ManagementDocument39 paginiGlycemic ManagementZayar HmunÎncă nu există evaluări
- GTT My PresentationDocument33 paginiGTT My PresentationSrikrishnaÎncă nu există evaluări
- ch In class PN complications case w Tony CHF (1)Document4 paginich In class PN complications case w Tony CHF (1)yairegtz2Încă nu există evaluări
- Inpatient DM MX in Twenty First CenturyDocument65 paginiInpatient DM MX in Twenty First CenturyTRP TSYOÎncă nu există evaluări
- Q Oral Glucose Tolerance TestDocument4 paginiQ Oral Glucose Tolerance TestNur Amirah FarhanahÎncă nu există evaluări
- TPN Origin and CalculationsDocument42 paginiTPN Origin and CalculationsmajdÎncă nu există evaluări
- Glucose Tolerance Test: Prakash MishraDocument31 paginiGlucose Tolerance Test: Prakash MishraRoyal LibraryÎncă nu există evaluări
- Endocrinology - Review NotesDocument9 paginiEndocrinology - Review NotesRoa Al-SajjanÎncă nu există evaluări
- Treating Diabetes: Dr. S. P. Mathew M. D. (Med) Ashok HospitalDocument57 paginiTreating Diabetes: Dr. S. P. Mathew M. D. (Med) Ashok HospitalMathew S Peedikayil100% (1)
- Stanford Hospital & Clinics Antimicrobial Dosing Reference Guide 2013Document3 paginiStanford Hospital & Clinics Antimicrobial Dosing Reference Guide 2013SANCHOSKYÎncă nu există evaluări
- Insulin Infustion OrdersDocument1 paginăInsulin Infustion Orderserma wanda mundariÎncă nu există evaluări
- GDM Screening Test and ManagementDocument5 paginiGDM Screening Test and ManagementTan Yuet YangÎncă nu există evaluări
- Insulin TherapyDocument23 paginiInsulin TherapyEliana MuisÎncă nu există evaluări
- Department of Biochemistry: Mrs. Bandanatham Aruna BIL2324338390/UMR0001280787 18-Feb-24 08:01 PMDocument1 paginăDepartment of Biochemistry: Mrs. Bandanatham Aruna BIL2324338390/UMR0001280787 18-Feb-24 08:01 PMChintha SreekanthÎncă nu există evaluări
- Augmentin DdsDocument11 paginiAugmentin DdsPrashanthBhatÎncă nu există evaluări
- Long Case - Initiation - Titration and Intensification Basal Insulin Therapy - Prandial InsulinDocument27 paginiLong Case - Initiation - Titration and Intensification Basal Insulin Therapy - Prandial InsulinRizqa FauziÎncă nu există evaluări
- Catatan GDS Dan TTVDocument2 paginiCatatan GDS Dan TTVAndi WijayaÎncă nu există evaluări
- GentamiciniDocument11 paginiGentamiciniBenjie SisonÎncă nu există evaluări
- Clinical Guidance On Diabetes Management at COVID-19 Patient Management FacilityDocument14 paginiClinical Guidance On Diabetes Management at COVID-19 Patient Management FacilitynrhmhealthÎncă nu există evaluări
- Insulin Sliding Scale ProtocolDocument2 paginiInsulin Sliding Scale ProtocolnashqonashÎncă nu există evaluări
- NTP MOP 6th Ed Module 5 Treatment of Drug Susceptible TB 10.20.20Document48 paginiNTP MOP 6th Ed Module 5 Treatment of Drug Susceptible TB 10.20.20gbÎncă nu există evaluări
- Ketogenic Diet "Yes & No" Guide For BeginnersDe la EverandKetogenic Diet "Yes & No" Guide For BeginnersEvaluare: 3 din 5 stele3/5 (1)
- Dimensional Analysis For Nursing StudentsDe la EverandDimensional Analysis For Nursing StudentsÎncă nu există evaluări
- Drug Allergy Skin Test, Test Dose, Desensitization AAAAI 2014 PDFDocument35 paginiDrug Allergy Skin Test, Test Dose, Desensitization AAAAI 2014 PDFWeeranan Sueb-LaÎncă nu există evaluări
- Genome CancerDocument8 paginiGenome CancerWeeranan Sueb-LaÎncă nu există evaluări
- Coding Manual For Case-Control Studies: SelectionDocument4 paginiCoding Manual For Case-Control Studies: Selectiondr_gentel19Încă nu există evaluări
- Newcastle OttawaDocument3 paginiNewcastle OttawaNovriefta NugrahaÎncă nu există evaluări
- Kdigo 2012 CKD GLDocument163 paginiKdigo 2012 CKD GLOkky Sari Rahayu100% (1)
- Acne Guideline 2016Document62 paginiAcne Guideline 2016Weeranan Sueb-LaÎncă nu există evaluări
- Oral FormulationsDocument10 paginiOral FormulationsSiddhartha MuppallaÎncă nu există evaluări
- HypothyrodismDocument1 paginăHypothyrodismkabal321Încă nu există evaluări
- Diabetic KetoacidosisDocument10 paginiDiabetic KetoacidosisdhanasundariÎncă nu există evaluări
- DIABETES MELLITUS SIGNS AND SYMPTOMSDocument3 paginiDIABETES MELLITUS SIGNS AND SYMPTOMSMutiara yunitaÎncă nu există evaluări
- ABG ExamplesDocument31 paginiABG ExamplesKEROLOS MAHROUSÎncă nu există evaluări
- QuizDocument8 paginiQuizTareq EmadÎncă nu există evaluări
- Acute Complication of Diabetic MellitusDocument10 paginiAcute Complication of Diabetic MellitusNdzalama Freedom MakhuveleÎncă nu există evaluări
- Diabetes EssayDocument3 paginiDiabetes Essaygreenharper100% (2)
- Case ReportDocument10 paginiCase ReportFika Wilda AnggraeniÎncă nu există evaluări
- Study Literatur: Pengkajian Luka Kaki DiabetesDocument15 paginiStudy Literatur: Pengkajian Luka Kaki DiabetesoctaviamayvikaÎncă nu există evaluări
- BHC Drug StudyDocument2 paginiBHC Drug StudyLeah Reese VersonÎncă nu există evaluări
- Cliinical Chemistry 1 (MKEB 2404)Document3 paginiCliinical Chemistry 1 (MKEB 2404)kiedd_04Încă nu există evaluări
- 1 s2.0 S2058534919301519 MainDocument5 pagini1 s2.0 S2058534919301519 MainjhuyÎncă nu există evaluări
- Synapse Diabetes Mellitus 5thDocument44 paginiSynapse Diabetes Mellitus 5thShihab100% (1)
- Nursing Care Plan No. 1 Assessment Diagnosis Planning Implementation Rationale Evaluation Subjective Data: Independent: IndependentDocument5 paginiNursing Care Plan No. 1 Assessment Diagnosis Planning Implementation Rationale Evaluation Subjective Data: Independent: Independentzebzeb STEMAÎncă nu există evaluări
- Lab ReportDocument2 paginiLab ReportSamir Kumar DashÎncă nu există evaluări
- Keseimbangan Asam Basa: Acid Base Balance - ARL 1Document43 paginiKeseimbangan Asam Basa: Acid Base Balance - ARL 1Ahmad MuttaqimÎncă nu există evaluări
- Prevalence of Gestational Diabetes and Contributing Factors Among Pregnant Jordanian Women Attending Jordan University HospitalDocument8 paginiPrevalence of Gestational Diabetes and Contributing Factors Among Pregnant Jordanian Women Attending Jordan University HospitalManar ShamielhÎncă nu există evaluări
- Acute Complication of Diabetes MellitusDocument37 paginiAcute Complication of Diabetes MellitusImron RosyadiÎncă nu există evaluări
- HHNS R.kalaivaniDocument14 paginiHHNS R.kalaivaniKalaivaany RamachandranÎncă nu există evaluări
- Adult Body Mass Index (BMI) Chart: WeightDocument2 paginiAdult Body Mass Index (BMI) Chart: WeightAshik AhmedÎncă nu există evaluări
- The Other Diabetes - LADA, or Type 1Document3 paginiThe Other Diabetes - LADA, or Type 1rey_fremyÎncă nu există evaluări
- PCOSQuestionnaire PDFDocument1 paginăPCOSQuestionnaire PDFRicha KohliÎncă nu există evaluări
- ENDO SamsonDocument12 paginiENDO SamsonMuhammad BilalÎncă nu există evaluări
- Case 1 ICCU CHARTDocument107 paginiCase 1 ICCU CHARTMaria Charis Anne IndananÎncă nu există evaluări
- School Name School ID 400224: (For All Grade Levels)Document1 paginăSchool Name School ID 400224: (For All Grade Levels)ynid wageÎncă nu există evaluări
- Obesity and Type 2 DiabetesDocument18 paginiObesity and Type 2 DiabetespritaultimardianÎncă nu există evaluări
- Thyroidism Patient Survey ResultsDocument90 paginiThyroidism Patient Survey ResultsBvayÎncă nu există evaluări
- Pengenalan DiabetesDocument57 paginiPengenalan DiabetesAsma MandaÎncă nu există evaluări
- Honk (Hiporosmolar Non Ketotik)Document24 paginiHonk (Hiporosmolar Non Ketotik)Raja Alfian IrawanÎncă nu există evaluări
- This Study Resource Was: Case Study 52: Cushing Syndrome Sara SauersDocument2 paginiThis Study Resource Was: Case Study 52: Cushing Syndrome Sara SauersJoshua del PozoÎncă nu există evaluări