S-ar putea să vă placă și
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5795)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Differentiation Questions and AnswerDocument10 paginiDifferentiation Questions and AnswerNazurah Kamaruzzaman KamariÎncă nu există evaluări
- The Zwolftonspiel of Josef Matthias Hauer: John RDocument36 paginiThe Zwolftonspiel of Josef Matthias Hauer: John RMax Kühn100% (1)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- BS 131-7-1998Document21 paginiBS 131-7-1998Germán VSÎncă nu există evaluări
- Dashboard Design Best PracticesDocument43 paginiDashboard Design Best Practicesgabriel_babiano8003100% (4)
- Safety Alarms Chiller and StarterDocument5 paginiSafety Alarms Chiller and StarterRaghavendra KaleÎncă nu există evaluări
- Earths InteriorDocument50 paginiEarths InteriorJulius Memeg PanayoÎncă nu există evaluări
- Chapter7 DigitalData 2Document217 paginiChapter7 DigitalData 2orizaÎncă nu există evaluări
- Research Methodology PDFDocument338 paginiResearch Methodology PDFBruno H Linhares PÎncă nu există evaluări
- Interview Q SASDocument43 paginiInterview Q SAShimaÎncă nu există evaluări
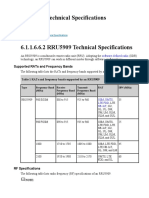
- RRU5909 Technical SpecificationsDocument7 paginiRRU5909 Technical SpecificationsDmitry059100% (1)
- Kidney Aging Sullivan 2016Document14 paginiKidney Aging Sullivan 2016Doni Andika PutraÎncă nu există evaluări
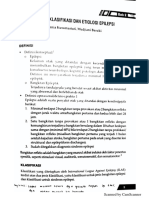
- EpilepsiDocument30 paginiEpilepsiDoni Andika PutraÎncă nu există evaluări
- Exercise 1Document5 paginiExercise 1Doni Andika PutraÎncă nu există evaluări
- Words in The News and Kunci Jawaban Exercise 1Document5 paginiWords in The News and Kunci Jawaban Exercise 1Doni Andika PutraÎncă nu există evaluări
- Chemistry Summary: Back To SchoolDocument25 paginiChemistry Summary: Back To SchoolDoni Andika PutraÎncă nu există evaluări
- FotoDocument1 paginăFotoDoni Andika PutraÎncă nu există evaluări
- SMAC Actuators User ManualDocument52 paginiSMAC Actuators User ManualGabo DuarÎncă nu există evaluări
- Compacted Graphite Iron - Mechanical and Physical Properties For Engine DesignDocument22 paginiCompacted Graphite Iron - Mechanical and Physical Properties For Engine DesignThanhluan NguyenÎncă nu există evaluări
- 2 EesyllDocument77 pagini2 EesyllDileepÎncă nu există evaluări
- Inductive Sensor For Temperature Measurement in Induction Heating Applications PDFDocument8 paginiInductive Sensor For Temperature Measurement in Induction Heating Applications PDFNjabulo XoloÎncă nu există evaluări
- Unit QuestionsDocument155 paginiUnit QuestionsSanya KhanÎncă nu există evaluări
- 支持允許多個 Vlan 的 Trunk 接口。: Techtalk/Td-P/58419Document6 pagini支持允許多個 Vlan 的 Trunk 接口。: Techtalk/Td-P/58419000-924680Încă nu există evaluări
- User AgentDocument2 paginiUser AgenthuongÎncă nu există evaluări
- Mass Transfer by Migration & Diffusion (Ch. 4)Document16 paginiMass Transfer by Migration & Diffusion (Ch. 4)Shekel DeninoÎncă nu există evaluări
- Basic Concepts in Biostatistics 1-1Document36 paginiBasic Concepts in Biostatistics 1-1Teslim RajiÎncă nu există evaluări
- Lecture Slides: Shigley's Mechanical Engineering DesignDocument95 paginiLecture Slides: Shigley's Mechanical Engineering DesignpurnaÎncă nu există evaluări
- BearingDocument4 paginiBearingJITENDRA BISWALÎncă nu există evaluări
- Ap Computer Science A Course OverviewDocument2 paginiAp Computer Science A Course Overviewbaojia chenÎncă nu există evaluări
- Compliance Statement - FormDocument16 paginiCompliance Statement - Formaqil khanÎncă nu există evaluări
- Servo Motor Application: Assignment - 2Document3 paginiServo Motor Application: Assignment - 2Smakshi ChoudharyÎncă nu există evaluări
- On Predicting Roller Milling Performance Part II. The Breakage FunctionDocument13 paginiOn Predicting Roller Milling Performance Part II. The Breakage FunctionKenneth AdamsÎncă nu există evaluări
- En 2014 New Brochure WebDocument20 paginiEn 2014 New Brochure WebSasa NackovicÎncă nu există evaluări
- Fuzzy Hungarian Method For Solving Intuitionistic FuzzyDocument7 paginiFuzzy Hungarian Method For Solving Intuitionistic Fuzzybima sentosaÎncă nu există evaluări
- Lebanese International University: CSCI 250 - Introduction To Programming - TEST-2: Student Name: Student IDDocument5 paginiLebanese International University: CSCI 250 - Introduction To Programming - TEST-2: Student Name: Student IDralf tamerÎncă nu există evaluări
- A Lightweight Secure Data Sharing SchemeDocument7 paginiA Lightweight Secure Data Sharing SchemeGopi KrishnaÎncă nu există evaluări
- Re - (Repeater-Builder) Midland Vehicular Repeater InfoDocument3 paginiRe - (Repeater-Builder) Midland Vehicular Repeater InfobbarinkÎncă nu există evaluări