S-ar putea să vă placă și
- Hipaa Authorization For Use or Disclosure of Health InformationDocument3 paginiHipaa Authorization For Use or Disclosure of Health InformationSalsabilla NurfaniaÎncă nu există evaluări
- D Iehp Consent FormDocument2 paginiD Iehp Consent Formapi-295326766Încă nu există evaluări
- Hipaa Authorization For Use or Disclosure of Health InformationDocument3 paginiHipaa Authorization For Use or Disclosure of Health InformationNigil josephÎncă nu există evaluări
- Records ReleaseDocument1 paginăRecords ReleaseChad MartinÎncă nu există evaluări
- Healthy LIC - Patient CONSENT Form EnglishDocument4 paginiHealthy LIC - Patient CONSENT Form EnglishTheFloatingHospitalÎncă nu există evaluări
- Authorization To Disclose Medical InformationDocument2 paginiAuthorization To Disclose Medical InformationFindLegalFormsÎncă nu există evaluări
- Psycho Social AssessmentDocument10 paginiPsycho Social Assessmentaa985rocketmailÎncă nu există evaluări
- Medical Power of Attorney TemplateDocument5 paginiMedical Power of Attorney Template5rprjnsd2bÎncă nu există evaluări
- Release of Infor FormDocument1 paginăRelease of Infor FormlostindallasÎncă nu există evaluări
- Detailed Medical Records HippaDocument1 paginăDetailed Medical Records HippaSergÎncă nu există evaluări
- Consent To Release InformationDocument2 paginiConsent To Release Informationkimmiej.gilbertÎncă nu există evaluări
- HIPAA Privacy Authorization Form: 2835 20 Street Vero Beach, FL 32960 Telephone: (772) 299-3003 Fax: (772) 299-3005Document3 paginiHIPAA Privacy Authorization Form: 2835 20 Street Vero Beach, FL 32960 Telephone: (772) 299-3003 Fax: (772) 299-3005api-104636361Încă nu există evaluări
- Authorization Form For Researchers The Use and Disclosure of PHIDocument2 paginiAuthorization Form For Researchers The Use and Disclosure of PHImatiushynsÎncă nu există evaluări
- JIT 2363 Authorization To Release Med RecordsDocument2 paginiJIT 2363 Authorization To Release Med Recordsalan benedettaÎncă nu există evaluări
- Sample HIE Consent 2020 Update FinalDocument1 paginăSample HIE Consent 2020 Update FinalKevin G. DavisÎncă nu există evaluări
- Release FormDocument1 paginăRelease FormRichard Dunn IIÎncă nu există evaluări
- 2 Hipaa Front Notices-Page 1 2-13Document1 pagină2 Hipaa Front Notices-Page 1 2-13api-214017719Încă nu există evaluări
- Form MUST Be Completed Before Signing or Will Not Be ValidDocument2 paginiForm MUST Be Completed Before Signing or Will Not Be ValidMaddox SquareÎncă nu există evaluări
- Hipaa Release Form FloridaDocument3 paginiHipaa Release Form FloridaAlan WattsÎncă nu există evaluări
- Red Badge E-Pack: Health Care Power of AttorneyDocument2 paginiRed Badge E-Pack: Health Care Power of AttorneyHigh Country Fire-Rescue Dept.Încă nu există evaluări
- Ambulance Signature FormDocument1 paginăAmbulance Signature FormVer BautistaÎncă nu există evaluări
- Standard Medical Power of Attorney Templates - LegalDocument4 paginiStandard Medical Power of Attorney Templates - LegalNancy CamussoÎncă nu există evaluări
- Innacle: Authorization To Receive or Release Medical InformationDocument2 paginiInnacle: Authorization To Receive or Release Medical InformationFrank ZÎncă nu există evaluări
- Generic Med Recs AuthDocument1 paginăGeneric Med Recs AuthmedonemedicalÎncă nu există evaluări
- Consent To Release Personal and Medical Information: Please Initial Beside Each Applicable DocumentDocument1 paginăConsent To Release Personal and Medical Information: Please Initial Beside Each Applicable DocumentMark Julius CabasanÎncă nu există evaluări
- Judicial Claims ClauseDocument2 paginiJudicial Claims ClauserubenguzÎncă nu există evaluări
- Medical Release Form 27 PDFDocument2 paginiMedical Release Form 27 PDFDina Dwi RamadhaniÎncă nu există evaluări
- Hipaa 1Document1 paginăHipaa 1Gregory KnispelÎncă nu există evaluări
- Release of InformationDocument2 paginiRelease of Informationxstn15Încă nu există evaluări
- HIPAA Release FormDocument3 paginiHIPAA Release FormBecky King FennerÎncă nu există evaluări
- Full Spectrum Health, LCC: Notice of Privacy Practices Acknowledgment FormDocument1 paginăFull Spectrum Health, LCC: Notice of Privacy Practices Acknowledgment FormTracey WieseÎncă nu există evaluări
- Medical Power of Attorney FormDocument5 paginiMedical Power of Attorney Formcmsvillar96Încă nu există evaluări
- Sample Consent 2020 Update FinalDocument1 paginăSample Consent 2020 Update FinalKevin G. DavisÎncă nu există evaluări
- Limited Power of AttorneyDocument5 paginiLimited Power of AttorneyKrite BanggawanÎncă nu există evaluări
- Official Medical Information and Release FormDocument2 paginiOfficial Medical Information and Release FormtheNOLAtreeÎncă nu există evaluări
- Advance Directive FormDocument4 paginiAdvance Directive FormMaimoon AliÎncă nu există evaluări
- Courtyard Pharmacy Form 9.15.2020Document1 paginăCourtyard Pharmacy Form 9.15.2020Mike EllmanÎncă nu există evaluări
- Caregiver AffidavitDocument4 paginiCaregiver AffidavitDougNewÎncă nu există evaluări
- 21GEN1212 Informed Consent - Minor - Covid EngDocument1 pagină21GEN1212 Informed Consent - Minor - Covid EngLaila PalmerÎncă nu există evaluări
- RqstRestrictionHealthInfoDocument1 paginăRqstRestrictionHealthInfocig3fÎncă nu există evaluări
- Lincoln Financial Authorization To Release InformationDocument1 paginăLincoln Financial Authorization To Release InformationSDÎncă nu există evaluări
- Authorization For Release of Medical RecordsDocument2 paginiAuthorization For Release of Medical RecordsEdward SnyderÎncă nu există evaluări
- P.I. Client Demand PackageDocument6 paginiP.I. Client Demand PackageDrew BallÎncă nu există evaluări
- Privacy AcknowledgementDocument1 paginăPrivacy Acknowledgementharrisk31Încă nu există evaluări
- Advocare Consent Disclosure Authorization PDFDocument2 paginiAdvocare Consent Disclosure Authorization PDFAsnaifa Bint MamintalÎncă nu există evaluări
- W A M R P ?: HAT RE Y Ights As A ArticipantDocument3 paginiW A M R P ?: HAT RE Y Ights As A ArticipantJack TedescoÎncă nu există evaluări
- Pursuant To The Health Insurance Portability and Accountability Act "HIPAA" of 4/14/03Document1 paginăPursuant To The Health Insurance Portability and Accountability Act "HIPAA" of 4/14/03cmferrer2005Încă nu există evaluări
- SLMC-English-TELEHEALTH CONSENT FORMDocument3 paginiSLMC-English-TELEHEALTH CONSENT FORMyio16711Încă nu există evaluări
- Authorization Form MedicalDocument1 paginăAuthorization Form Medicalapi-207296970Încă nu există evaluări
- Authorization 14896248Document2 paginiAuthorization 14896248Darrel HeathÎncă nu există evaluări
- YawaconsentmediaDocument3 paginiYawaconsentmediaapi-327205829Încă nu există evaluări
- Youth Department Permission FormDocument2 paginiYouth Department Permission FormhillatchapelhillÎncă nu există evaluări
- QR-RCP-009 Authorization For Disclosure of Health InformationRecords - Rev07Document1 paginăQR-RCP-009 Authorization For Disclosure of Health InformationRecords - Rev07Yel BÎncă nu există evaluări
- Texas Statutory Durable Power of AttorneyDocument3 paginiTexas Statutory Durable Power of Attorneyc3praiseÎncă nu există evaluări
- Consent For Participation To PhieDocument1 paginăConsent For Participation To PhiebenÎncă nu există evaluări
- Arkansas Durable Medical Power of Attorney FormDocument3 paginiArkansas Durable Medical Power of Attorney FormTiara HamiltonÎncă nu există evaluări
- TEMPLATE Medical Release WITHOUT Notary 1Document1 paginăTEMPLATE Medical Release WITHOUT Notary 1Peter WagnerÎncă nu există evaluări
- Patient Registration Form: General Information (Please Print Neatly)Document5 paginiPatient Registration Form: General Information (Please Print Neatly)Dan ThomasÎncă nu există evaluări
- Durable - Power - of - Attorney 1Document5 paginiDurable - Power - of - Attorney 1cjÎncă nu există evaluări
- Cross-Training: The Medical Assistant WorkbookDe la EverandCross-Training: The Medical Assistant WorkbookÎncă nu există evaluări
- Jurnal Job DescriptionDocument13 paginiJurnal Job DescriptionAji Mulia PrasÎncă nu există evaluări
- Abnt NBR 16868 1 Alvenaria Estrutural ProjetoDocument77 paginiAbnt NBR 16868 1 Alvenaria Estrutural ProjetoGIOVANNI BRUNO COELHO DE PAULAÎncă nu există evaluări
- Amity School of Business:, Semester IV Research Methodology and Report Preparation Dr. Deepa KapoorDocument23 paginiAmity School of Business:, Semester IV Research Methodology and Report Preparation Dr. Deepa KapoorMayank TayalÎncă nu există evaluări
- Taylor Series PDFDocument147 paginiTaylor Series PDFDean HaynesÎncă nu există evaluări
- 1188 2665 1 SMDocument12 pagini1188 2665 1 SMRita BangunÎncă nu există evaluări
- Installation Instructions INI Luma Gen2Document21 paginiInstallation Instructions INI Luma Gen2John Kim CarandangÎncă nu există evaluări
- Levels of CommunicationDocument3 paginiLevels of CommunicationAiyaz ShaikhÎncă nu există evaluări
- 5620 SAM Rel 14 License Point Configuration ToolDocument416 pagini5620 SAM Rel 14 License Point Configuration Toolluis100% (1)
- Leveriza Heights SubdivisionDocument4 paginiLeveriza Heights SubdivisionTabordan AlmaeÎncă nu există evaluări
- Log and Antilog TableDocument3 paginiLog and Antilog TableDeboshri BhattacharjeeÎncă nu există evaluări
- BSS Troubleshooting Manual PDFDocument220 paginiBSS Troubleshooting Manual PDFleonardomarinÎncă nu există evaluări
- Radio Ac DecayDocument34 paginiRadio Ac DecayQassem MohaidatÎncă nu există evaluări
- Industrial ReportDocument52 paginiIndustrial ReportSiddharthÎncă nu există evaluări
- Core CompetenciesDocument3 paginiCore Competenciesapi-521620733Încă nu există evaluări
- Electronic Diversity Visa ProgrambDocument1 paginăElectronic Diversity Visa Programbsamkimari5Încă nu există evaluări
- Sheet-Metal Forming Processes: Group 9 PresentationDocument90 paginiSheet-Metal Forming Processes: Group 9 PresentationjssrikantamurthyÎncă nu există evaluări
- Control ValvesDocument95 paginiControl ValvesHardik Acharya100% (1)
- Object Oriented ParadigmDocument2 paginiObject Oriented ParadigmDickson JohnÎncă nu există evaluări
- Problem Solving No. 123Document5 paginiProblem Solving No. 123Christy Joy BarboÎncă nu există evaluări
- Atoma Amd Mol&Us CCTK) : 2Nd ErmDocument4 paginiAtoma Amd Mol&Us CCTK) : 2Nd ErmjanviÎncă nu există evaluări
- (EN 10348) - Steel For The Reinforcement of Concrete. Galvanized Reinforcing SteelDocument24 pagini(EN 10348) - Steel For The Reinforcement of Concrete. Galvanized Reinforcing Steelbagusu_6Încă nu există evaluări
- Management Accounting by Cabrera Solution Manual 2011 PDFDocument3 paginiManagement Accounting by Cabrera Solution Manual 2011 PDFClaudette Clemente100% (1)
- I. Choose The Best Option (From A, B, C or D) To Complete Each Sentence: (3.0pts)Document5 paginiI. Choose The Best Option (From A, B, C or D) To Complete Each Sentence: (3.0pts)thmeiz.17sÎncă nu există evaluări
- Anker Soundcore Mini, Super-Portable Bluetooth SpeakerDocument4 paginiAnker Soundcore Mini, Super-Portable Bluetooth SpeakerM.SaadÎncă nu există evaluări
- Calculating Free Energies Using Adaptive Biasing Force MethodDocument14 paginiCalculating Free Energies Using Adaptive Biasing Force MethodAmin SagarÎncă nu există evaluări
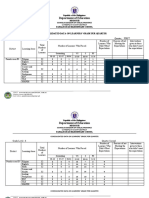
- Department of Education: Consolidated Data On Learners' Grade Per QuarterDocument4 paginiDepartment of Education: Consolidated Data On Learners' Grade Per QuarterUsagi HamadaÎncă nu există evaluări
- The Bio-Based Economy in The NetherlandsDocument12 paginiThe Bio-Based Economy in The NetherlandsIrving Toloache FloresÎncă nu există evaluări
- G.Devendiran: Career ObjectiveDocument2 paginiG.Devendiran: Career ObjectiveSadha SivamÎncă nu există evaluări
- D E S C R I P T I O N: Acknowledgement Receipt For EquipmentDocument2 paginiD E S C R I P T I O N: Acknowledgement Receipt For EquipmentTindusNiobetoÎncă nu există evaluări
- LG LFX31945 Refrigerator Service Manual MFL62188076 - Signature2 Brand DID PDFDocument95 paginiLG LFX31945 Refrigerator Service Manual MFL62188076 - Signature2 Brand DID PDFplasmapete71% (7)