S-ar putea să vă placă și
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- Cardiac Surgery MCQDocument43 paginiCardiac Surgery MCQprofarmah100% (7)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- Research Article Investigation of Effects of Terpene Skin Penetration Enhancers On Stability and Biological Activity of LysozymeDocument7 paginiResearch Article Investigation of Effects of Terpene Skin Penetration Enhancers On Stability and Biological Activity of LysozymeNur Camelia PragnandaÎncă nu există evaluări
- 10 1080@14764172 2017 1368666Document30 pagini10 1080@14764172 2017 1368666Nur Camelia PragnandaÎncă nu există evaluări
- Long Term Outcome of Secondary Glaucoma Following Vitreoretinal SurgeryDocument3 paginiLong Term Outcome of Secondary Glaucoma Following Vitreoretinal SurgeryNur Camelia PragnandaÎncă nu există evaluări
- Effect of Head and Body Position On Intraocular PressureDocument5 paginiEffect of Head and Body Position On Intraocular PressureNur Camelia PragnandaÎncă nu există evaluări
- Safety Environment and Bed Making (Group 5)Document6 paginiSafety Environment and Bed Making (Group 5)Mira AurumtinÎncă nu există evaluări
- Advice Following Nasal Surgery Fes Sep20Document8 paginiAdvice Following Nasal Surgery Fes Sep20Adela MarcovÎncă nu există evaluări
- Antimicrobial FinalDocument227 paginiAntimicrobial FinalAbdulrhman MekawyÎncă nu există evaluări
- Pengaruh Massage Kaki Terhadap Penurunan Insomnia Pada Lansia Di Banjar Temesi Desa Temesi Kabupaten GianyarDocument12 paginiPengaruh Massage Kaki Terhadap Penurunan Insomnia Pada Lansia Di Banjar Temesi Desa Temesi Kabupaten Gianyar119 CIKOKOLÎncă nu există evaluări
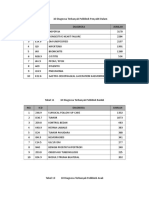
- 10 Diagnosa PenyakitDocument3 pagini10 Diagnosa PenyakitDiny Rachma Putri HÎncă nu există evaluări
- Week 4 Bio Lab 7/28/2012Document2 paginiWeek 4 Bio Lab 7/28/2012KT100% (1)
- Pharma - 2020 General Principles of Drug ActionDocument163 paginiPharma - 2020 General Principles of Drug Actiongelean payodÎncă nu există evaluări
- AppendicitisDocument11 paginiAppendicitisbobtagubaÎncă nu există evaluări
- Pharmacy Journals 100Document7 paginiPharmacy Journals 100alexpharmÎncă nu există evaluări
- How To CPR PDFDocument133 paginiHow To CPR PDFandrinjoÎncă nu există evaluări
- Bragdon V AbbottDocument22 paginiBragdon V AbbottZÎncă nu există evaluări
- Nursing Care To Promote Fetal and Maternal HealthDocument4 paginiNursing Care To Promote Fetal and Maternal HealthKristine BartsÎncă nu există evaluări
- Therapeutic UltrasoundDocument18 paginiTherapeutic UltrasoundPhysio Ebook100% (1)
- Phlebotomy TechnacianDocument1 paginăPhlebotomy Technacianapi-78318377Încă nu există evaluări
- Can Trees Get CancerDocument2 paginiCan Trees Get CancerSimarpreet Kaur 1025Încă nu există evaluări
- Pharmaceutical Biotechnology-QBDocument8 paginiPharmaceutical Biotechnology-QBprateekshaÎncă nu există evaluări
- Case Study 1 - Mrs. SmithDocument3 paginiCase Study 1 - Mrs. SmithJulia CooperÎncă nu există evaluări
- Ajor Epressive Isorder: Marshall Cates, Angela Passero, and Jacqueline FeldmanDocument16 paginiAjor Epressive Isorder: Marshall Cates, Angela Passero, and Jacqueline FeldmanbencleeseÎncă nu există evaluări
- Asking Reporting Health Problems & Diagnosing: OlehDocument5 paginiAsking Reporting Health Problems & Diagnosing: Olehsindimei alvianiÎncă nu există evaluări
- How A Breath Is Delivered: OutlineDocument16 paginiHow A Breath Is Delivered: OutlineLesly Peinado TorresÎncă nu există evaluări
- Auricular Causative Diagnosis-Finding The Roots of Diseases: A Study of Clinical CasesDocument11 paginiAuricular Causative Diagnosis-Finding The Roots of Diseases: A Study of Clinical Casesyan92120Încă nu există evaluări
- Refractive ErrorsDocument15 paginiRefractive ErrorsMubasher 783Încă nu există evaluări
- Tonsillectomy and Adenoidectomy - Pediatric Clinics of North AmericaDocument13 paginiTonsillectomy and Adenoidectomy - Pediatric Clinics of North AmericayosefÎncă nu există evaluări
- Format of Medical Certificate-AlpDocument3 paginiFormat of Medical Certificate-AlpXII C 38 DEVANAND T AÎncă nu există evaluări
- GE Healthcare AnestesiaDocument128 paginiGE Healthcare AnestesiaLuis Alberto Jiménez AcataÎncă nu există evaluări
- Perforasi Pada Penderita Apendisitis Di RSUD DR.H.Abdul Moeloek LampungDocument7 paginiPerforasi Pada Penderita Apendisitis Di RSUD DR.H.Abdul Moeloek LampungKikiÎncă nu există evaluări
- Lap Ok RSGM Ronal HudaDocument23 paginiLap Ok RSGM Ronal HudaDwi SastrawanÎncă nu există evaluări
- Baking Soda A Cure For HumanityDocument6 paginiBaking Soda A Cure For Humanitysheriff77080% (5)
- Inistitutional Assessementknowledge Test For Comprhenssive NursingDocument19 paginiInistitutional Assessementknowledge Test For Comprhenssive NursingkassahunÎncă nu există evaluări