S-ar putea să vă placă și
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Optimal Shoulder Performance - Cressey ReinoldDocument40 paginiOptimal Shoulder Performance - Cressey ReinoldPricope Madalina93% (14)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- Mechanics 1 Test 10 - 11 AnswersDocument23 paginiMechanics 1 Test 10 - 11 AnswersPaul Burgess50% (2)
- Mansions of Madness Second Editon Rules ReferenceDocument24 paginiMansions of Madness Second Editon Rules ReferenceGeorge AlexandrisÎncă nu există evaluări
- Fabian Von Auerswald PDFDocument2 paginiFabian Von Auerswald PDFAmyÎncă nu există evaluări
- 01 To 15 AUGUST GAURAV BHAI DAILY PDFDocument508 pagini01 To 15 AUGUST GAURAV BHAI DAILY PDFrupaÎncă nu există evaluări
- November 2017 Month in ReviewDocument2 paginiNovember 2017 Month in ReviewEmily KaderÎncă nu există evaluări
- JEP Journal of Exercise PhysiologyDocument7 paginiJEP Journal of Exercise PhysiologykambuaÎncă nu există evaluări
- A Ball Player's Career Being The Personal Experiences and Reminiscensces of Adrian C. Anson by Anson, Adrian Constantine, 1852-1922Document171 paginiA Ball Player's Career Being The Personal Experiences and Reminiscensces of Adrian C. Anson by Anson, Adrian Constantine, 1852-1922Gutenberg.orgÎncă nu există evaluări
- Learning Activity 3: Fuente: SENADocument3 paginiLearning Activity 3: Fuente: SENAjairo andres vargas ruedaÎncă nu există evaluări
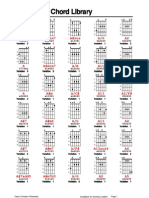
- SongBase Chord LibraryDocument22 paginiSongBase Chord LibraryHenry GarzónÎncă nu există evaluări
- Keesha - Barney Wiki - FandomDocument5 paginiKeesha - Barney Wiki - FandomchefchadsmithÎncă nu există evaluări
- Artikel Bahasa Inggris Tentang Kesehatan IDocument3 paginiArtikel Bahasa Inggris Tentang Kesehatan IRestu Yogi Fahlevi100% (2)
- Arcade FB Neo RL Plus 2.1Document116 paginiArcade FB Neo RL Plus 2.1Sonia García FernándezÎncă nu există evaluări
- Hope - 1 Grade 11: Exercise For FitnessDocument6 paginiHope - 1 Grade 11: Exercise For FitnessTABBAL JAN PAOLOÎncă nu există evaluări
- Coaching Diversity: The Rooney Rule, Its Application and Ideas For ExpansionDocument10 paginiCoaching Diversity: The Rooney Rule, Its Application and Ideas For Expansionbear clawÎncă nu există evaluări
- Fitness His Edition JulyAugust 2017Document84 paginiFitness His Edition JulyAugust 2017Afzal FeerestaÎncă nu există evaluări
- D&D 3e - Tiles - Battlemaps - Dungeon Rooms Vol VIDocument27 paginiD&D 3e - Tiles - Battlemaps - Dungeon Rooms Vol VIRuppert Smooker Jr.100% (1)
- CB Golf 2010 2011Document89 paginiCB Golf 2010 2011mail_markhawleyÎncă nu există evaluări
- How To Slipstream All Intel SATA Drivers With XPDocument12 paginiHow To Slipstream All Intel SATA Drivers With XPBirendra Kumar SinghÎncă nu există evaluări
- Popular MechanicsDocument132 paginiPopular MechanicsRaviChandra100% (7)
- Valten, Exalted of SigmarDocument1 paginăValten, Exalted of SigmarpodkinpoÎncă nu există evaluări
- Ing GrisDocument5 paginiIng GrisChristy TheresaÎncă nu există evaluări
- Guitar PartsDocument15 paginiGuitar Partsaftersound bandÎncă nu există evaluări
- Momets QPDocument8 paginiMomets QPErtuğ ÖzyiğitÎncă nu există evaluări
- Mercedes BenzDocument22 paginiMercedes BenzYusra SayedÎncă nu există evaluări
- IC4 L2 WQ U3to4Document2 paginiIC4 L2 WQ U3to4Elia BidiakÎncă nu există evaluări
- ARTHRITISDocument12 paginiARTHRITISram krishna100% (1)
- JMC 2024 Question PaperDocument4 paginiJMC 2024 Question Paperlayden.jp6932Încă nu există evaluări
- G4000Document24 paginiG4000AbuAhmedQuaziÎncă nu există evaluări
- Part Catalogue Yamaha YZF R25 2020 B4P1 MALAYSIADocument69 paginiPart Catalogue Yamaha YZF R25 2020 B4P1 MALAYSIAmhz myÎncă nu există evaluări