S-ar putea să vă placă și
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- All 13496Document15 paginiAll 13496Jaya Semara PutraÎncă nu există evaluări
- Chylothorax Diagnosis Review 2010Document7 paginiChylothorax Diagnosis Review 2010adriantiariÎncă nu există evaluări
- Treatment of Fungal Infections in Adult Pulmonary Critical Care and Sleep MedicineDocument33 paginiTreatment of Fungal Infections in Adult Pulmonary Critical Care and Sleep MedicineIsabel Suni Jimenez CasaverdeÎncă nu există evaluări
- CommunityDocument11 paginiCommunityJaya Semara PutraÎncă nu există evaluări
- Lung Hyperinflation in COPD: Applying Physiology To Clinical PracticeDocument12 paginiLung Hyperinflation in COPD: Applying Physiology To Clinical PracticeJaya Semara PutraÎncă nu există evaluări
- Recurrent Unilateral Pleural Effusion From Constrictive Pericarditis of Unknown Etiology Requiring PericardiectomyDocument3 paginiRecurrent Unilateral Pleural Effusion From Constrictive Pericarditis of Unknown Etiology Requiring PericardiectomyJaya Semara PutraÎncă nu există evaluări
- LastDocument3 paginiLastJaya Semara PutraÎncă nu există evaluări
- DC in Priming T CellDocument8 paginiDC in Priming T CellJaya Semara PutraÎncă nu există evaluări
- Unilateral Post TB Destroy LungDocument3 paginiUnilateral Post TB Destroy LungJaya Semara PutraÎncă nu există evaluări
- Aztreonam: Antibiotic ClassDocument2 paginiAztreonam: Antibiotic ClassJaya Semara PutraÎncă nu există evaluări
- PE GuidelinesDocument12 paginiPE GuidelinesJaya Semara PutraÎncă nu există evaluări
- Aquickreferenceon Respiratoryacidosis: Rebecca A. JohnsonDocument5 paginiAquickreferenceon Respiratoryacidosis: Rebecca A. JohnsonJaya Semara PutraÎncă nu există evaluări
- Bubble Trouble A Review of Diving Physiology andDocument9 paginiBubble Trouble A Review of Diving Physiology andJaya Semara PutraÎncă nu există evaluări
- Page 1Document9 paginiPage 1Jaya Semara PutraÎncă nu există evaluări
- Mehl Horn 2007Document8 paginiMehl Horn 2007Jaya Semara PutraÎncă nu există evaluări
- Respiratory Medicine Case ReportsDocument3 paginiRespiratory Medicine Case ReportsJaya Semara PutraÎncă nu există evaluări
- Zhan El 2004Document7 paginiZhan El 2004Jaya Semara PutraÎncă nu există evaluări
- Distress Syndrome (ARDS) : Penggunaan Ventilasi Mekanis Invasif Pada Acute RespiratoryDocument9 paginiDistress Syndrome (ARDS) : Penggunaan Ventilasi Mekanis Invasif Pada Acute Respiratorydoktermuda91Încă nu există evaluări
- Post-Tuberculous Bronchiectasis: Indications For Surgical TreatmentDocument2 paginiPost-Tuberculous Bronchiectasis: Indications For Surgical TreatmentJaya Semara PutraÎncă nu există evaluări
- Pharmacodynamics of Antimicrobial Agents: Time-Dependent vs. Concentration-Dependent KillingDocument4 paginiPharmacodynamics of Antimicrobial Agents: Time-Dependent vs. Concentration-Dependent KillingMaddy AlbuletÎncă nu există evaluări
- Thoraxjnl 2015 208188Document6 paginiThoraxjnl 2015 208188Jaya Semara PutraÎncă nu există evaluări
- Streptococcus Suis Serotype 2-Induced Meningoencephalitis: Cerebral Abscesses in A Pig: Atypical Manifestations ofDocument5 paginiStreptococcus Suis Serotype 2-Induced Meningoencephalitis: Cerebral Abscesses in A Pig: Atypical Manifestations ofJaya Semara PutraÎncă nu există evaluări
- Necrotizing Pneumonia 1Document7 paginiNecrotizing Pneumonia 1Jaya Semara PutraÎncă nu există evaluări
- Bubble Trouble A Review of Diving Physiology andDocument9 paginiBubble Trouble A Review of Diving Physiology andJaya Semara PutraÎncă nu există evaluări
- Algrythm HypercalcemiaDocument7 paginiAlgrythm HypercalcemiaJaya Semara PutraÎncă nu există evaluări
- Respiratory Failure Mechanical VentilationDocument37 paginiRespiratory Failure Mechanical Ventilationawakepull312Încă nu există evaluări
- 1.BE Airway DefenseDocument11 pagini1.BE Airway DefenseJaya Semara PutraÎncă nu există evaluări
- 2.BE PathogenesisDocument7 pagini2.BE PathogenesisJaya Semara PutraÎncă nu există evaluări
- Distress Syndrome (ARDS) : Penggunaan Ventilasi Mekanis Invasif Pada Acute RespiratoryDocument9 paginiDistress Syndrome (ARDS) : Penggunaan Ventilasi Mekanis Invasif Pada Acute Respiratorydoktermuda91Încă nu există evaluări
- Lung Abscess Diagnosis, Etio, Treatment OptionDocument12 paginiLung Abscess Diagnosis, Etio, Treatment OptionJaya Semara PutraÎncă nu există evaluări
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Kode Kombinasi Icd 10 Dan Icd 9 Indonesia Update 2018Document10 paginiKode Kombinasi Icd 10 Dan Icd 9 Indonesia Update 2018Dini AzizahÎncă nu există evaluări
- Gastro MCQsDocument14 paginiGastro MCQsvaegmundigÎncă nu există evaluări
- Figo Staging Cancer CervicalDocument7 paginiFigo Staging Cancer CervicalihsansabridrÎncă nu există evaluări
- NCM 112 (FINALS) Chap 1Document2 paginiNCM 112 (FINALS) Chap 1MikasaÎncă nu există evaluări
- POULTRY PATHO - Marek's DiseaseDocument31 paginiPOULTRY PATHO - Marek's DiseaseArooma KhalidÎncă nu există evaluări
- Ventricular Septal DefectDocument16 paginiVentricular Septal DefectPai PAiÎncă nu există evaluări
- SOP Kids Club COVID 19 Measure For GO 2Document2 paginiSOP Kids Club COVID 19 Measure For GO 2adjcdaughtÎncă nu există evaluări
- Vigabatrin For IsDocument12 paginiVigabatrin For IsAndrew SantosoÎncă nu există evaluări
- Chapter #5 - Summary Abnormal Psychology: An Integrative Approach Chapter #5 - Summary Abnormal Psychology: An Integrative ApproachDocument13 paginiChapter #5 - Summary Abnormal Psychology: An Integrative Approach Chapter #5 - Summary Abnormal Psychology: An Integrative ApproachDjane VillarinÎncă nu există evaluări
- DefibrillationDocument9 paginiDefibrillationJara Maris Moreno BudionganÎncă nu există evaluări
- Case Study On Nephrotic SyndromeDocument7 paginiCase Study On Nephrotic SyndromeArchana VermaÎncă nu există evaluări
- Surgical Wound Classification Revision 2012Document1 paginăSurgical Wound Classification Revision 2012Hema Meliny Perangin-angin100% (1)
- World Rabies DayDocument6 paginiWorld Rabies DayZETTYÎncă nu există evaluări
- Digital Covid Questionnaire For Revival Approval FormatDocument2 paginiDigital Covid Questionnaire For Revival Approval Formatsouravdey3Încă nu există evaluări
- Brucellosis Brucellosis: Brucella Spp. Brucella SPPDocument24 paginiBrucellosis Brucellosis: Brucella Spp. Brucella SPPhussain AltaherÎncă nu există evaluări
- Iron Deficiency AnemiaDocument4 paginiIron Deficiency AnemiaWiljohn de la CruzÎncă nu există evaluări
- Paedia - Dr. RehabDocument173 paginiPaedia - Dr. RehabMohammed Saad NabhanÎncă nu există evaluări
- 114 okMSAD AFP-Differentiation and Diagnosis of Tremor PDFDocument6 pagini114 okMSAD AFP-Differentiation and Diagnosis of Tremor PDFkasmiantoabadiÎncă nu există evaluări
- Klinefelter Syndrome in Clinical Practice. Nat Clin Pract Urol 4:192-204Document14 paginiKlinefelter Syndrome in Clinical Practice. Nat Clin Pract Urol 4:192-204Anonymous LAWfm7Încă nu există evaluări
- Systematic Review Pelaksanaan Programmatic Management of Drug-Resistant Tuberculosis Pada Pasien Tuberkulosis Resistan ObatDocument8 paginiSystematic Review Pelaksanaan Programmatic Management of Drug-Resistant Tuberculosis Pada Pasien Tuberkulosis Resistan ObatAdinda Pramesthi RiadyaniÎncă nu există evaluări
- Evaluation of Macrocytic AnemiasDocument8 paginiEvaluation of Macrocytic Anemiasmy accountÎncă nu există evaluări
- JH CERILLES STATE COLLEGE - Post TestDocument7 paginiJH CERILLES STATE COLLEGE - Post TestCrystal Ann TadiamonÎncă nu există evaluări
- Kawasaki Disease Case ReportDocument17 paginiKawasaki Disease Case ReportAlvaro Villarejo PérezÎncă nu există evaluări
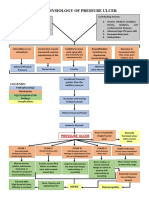
- Pathophysiology of Pressure UlcerDocument1 paginăPathophysiology of Pressure UlcerSTORAGE FILEÎncă nu există evaluări
- Kidney DiseasesDocument93 paginiKidney DiseasesDoreen NÎncă nu există evaluări
- Prevenção Secundária Avc Isquêmico - Guideline 2022Document41 paginiPrevenção Secundária Avc Isquêmico - Guideline 2022Felipe Stoquetti de AbreuÎncă nu există evaluări
- Bhatia and Speed Grand Test McqsDocument10 paginiBhatia and Speed Grand Test McqsRavi RajaÎncă nu există evaluări
- NGT Ogt-FeedingDocument14 paginiNGT Ogt-Feedingnibbles nibblesÎncă nu există evaluări
- THC AspergerDocument168 paginiTHC AspergerMICHAELÎncă nu există evaluări
- MCQ-Chronic Obstructive Pulmonary DiseaseDocument3 paginiMCQ-Chronic Obstructive Pulmonary DiseaseMittulÎncă nu există evaluări