S-ar putea să vă placă și
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- MAPEH 6 - Demo COTDocument36 paginiMAPEH 6 - Demo COTLucena GhieÎncă nu există evaluări
- A Guide To Field Notes For Qualitative Research: Context and ConversationDocument9 paginiA Guide To Field Notes For Qualitative Research: Context and Conversationfrente amplio animalistaÎncă nu există evaluări
- Nuclear Medical Technologist Medicine in Chicago IL Resume Marianne VanekDocument1 paginăNuclear Medical Technologist Medicine in Chicago IL Resume Marianne VanekMarianneVanekÎncă nu există evaluări
- Capa Plan 2018Document3 paginiCapa Plan 2018Cha Gabriel100% (2)
- Perineal Scar Endometriosis: Case ReportDocument4 paginiPerineal Scar Endometriosis: Case ReportMudassirÎncă nu există evaluări
- Role of Covering Ileostomy in Anastomotic StricturesDocument7 paginiRole of Covering Ileostomy in Anastomotic StricturesMudassirÎncă nu există evaluări
- Clinicopathological Profile of Colorectal Cancer in Kashmir PDFDocument5 paginiClinicopathological Profile of Colorectal Cancer in Kashmir PDFMudassirÎncă nu există evaluări
- Clinicopathological Profile of Colorectal Cancer in KashmirDocument5 paginiClinicopathological Profile of Colorectal Cancer in KashmirMudassirÎncă nu există evaluări
- Kunjungan Sakit CilinayaDocument56 paginiKunjungan Sakit CilinayaAji S WidodoÎncă nu există evaluări
- Journal of Applied Health Management and TechnologyDocument12 paginiJournal of Applied Health Management and Technologysalsabil vaniÎncă nu există evaluări
- NICU Booklet April2020Document90 paginiNICU Booklet April2020Popescu VioricaÎncă nu există evaluări
- The Effect of The Distance From The Contact Point To The Crystal Bone On The Degree of Vertical Loss of Interdental PapillaDocument5 paginiThe Effect of The Distance From The Contact Point To The Crystal Bone On The Degree of Vertical Loss of Interdental PapillaAlfred OrozcoÎncă nu există evaluări
- Implementasi Aseptik Dispensing Sesuai Standar PKPO SNARSDocument21 paginiImplementasi Aseptik Dispensing Sesuai Standar PKPO SNARSAkhmad Safi'iÎncă nu există evaluări
- National CPD Certificate Information and Guidance BookDocument22 paginiNational CPD Certificate Information and Guidance Bookmeenakshi.r.agrawalÎncă nu există evaluări
- List of Hospitals in UAEDocument7 paginiList of Hospitals in UAEaneebqualitasÎncă nu există evaluări
- Jurnal 2 Terapi Bedah - HDocument4 paginiJurnal 2 Terapi Bedah - HYusuf DiansyahÎncă nu există evaluări
- Food Handler Training CoursesDocument2 paginiFood Handler Training CoursesSai Ram ChanduriÎncă nu există evaluări
- Emergency First Initial Assesment: Monday, October 05, 2020Document50 paginiEmergency First Initial Assesment: Monday, October 05, 2020Agoes TreeyantÎncă nu există evaluări
- The Philippine Health ProblemDocument51 paginiThe Philippine Health ProblemZuleira ParraÎncă nu există evaluări
- Danafarber CancerDocument273 paginiDanafarber CanceriulianamileaÎncă nu există evaluări
- DHJ 26.04.23 Lengkap ADocument23 paginiDHJ 26.04.23 Lengkap AMalik TeamÎncă nu există evaluări
- Dental Officer Information - e (1989)Document10 paginiDental Officer Information - e (1989)Marian GarciaÎncă nu există evaluări
- Healthcare & Life Sciences ReviewDocument47 paginiHealthcare & Life Sciences Reviewmercadia59970% (1)
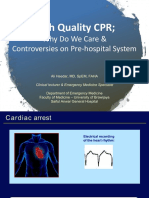
- High Quality CPR, DR Ali Haedar PDFDocument45 paginiHigh Quality CPR, DR Ali Haedar PDFTaufik SuhendarÎncă nu există evaluări
- Annual Report QF 2018 19Document57 paginiAnnual Report QF 2018 19Muhammad FaisalÎncă nu există evaluări
- 5 - Upper Limb Prosthetics Critical Factors in Device Abandonment - 2007Document11 pagini5 - Upper Limb Prosthetics Critical Factors in Device Abandonment - 2007Fernando PessoaÎncă nu există evaluări
- Melonorm CapsuleDocument3 paginiMelonorm Capsulehk_scribdÎncă nu există evaluări
- Laws That Maybe Related To Nursing PracticeDocument8 paginiLaws That Maybe Related To Nursing Practicealvin1317020009304100% (5)
- Science Citation Index Expanded - Dentistry, Oral Surgery & Medicine - Journal ListDocument17 paginiScience Citation Index Expanded - Dentistry, Oral Surgery & Medicine - Journal ListJelena JacimovicÎncă nu există evaluări
- Docs in PuneDocument238 paginiDocs in Punemenolove100% (1)
- Caregiver Resume ExamplesDocument7 paginiCaregiver Resume Examplesphewzeajd100% (2)
- (Medical Radiology) Lluís Donoso-Bach, Giles W. L. Boland - Quality and Safety in Imaging-Springer International Publishing (2018)Document187 pagini(Medical Radiology) Lluís Donoso-Bach, Giles W. L. Boland - Quality and Safety in Imaging-Springer International Publishing (2018)Piotr JankowskiÎncă nu există evaluări
- Our MissionDocument5 paginiOur MissionShohaib Khan TanoliÎncă nu există evaluări
- Airforce Career Feild BreakdownDocument1 paginăAirforce Career Feild BreakdownJoseph RobinsonÎncă nu există evaluări