S-ar putea să vă placă și
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Response Assessment in Neuro-OncologyDocument40 paginiResponse Assessment in Neuro-Oncologyimk_mithunÎncă nu există evaluări
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5795)
- Adhesive Capsulitis Presentation May 2009Document29 paginiAdhesive Capsulitis Presentation May 2009cm4100% (1)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Dr. Mohammed Shahedur Rahman Khan Bronchial Asthma Management Aspects - Current and FutureDocument32 paginiDr. Mohammed Shahedur Rahman Khan Bronchial Asthma Management Aspects - Current and FutureShahadat Hossain BabuÎncă nu există evaluări
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Final PhysicalDocument409 paginiFinal PhysicalAbhishiktaAbhiÎncă nu există evaluări
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- ABO-Rh Blood Typing With Synthetic Blood: Teacher'S Manual and Student GuideDocument32 paginiABO-Rh Blood Typing With Synthetic Blood: Teacher'S Manual and Student GuideMylan Gaston100% (1)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- IFM+Toolkit+Table+of+Contents v19Document13 paginiIFM+Toolkit+Table+of+Contents v19khaled dewanÎncă nu există evaluări
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Differences in Left Ventricular and Left Atrial FuDocument10 paginiDifferences in Left Ventricular and Left Atrial FueugeniaÎncă nu există evaluări
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- Bhoomi PatelDocument9 paginiBhoomi PatelPooja PanchalÎncă nu există evaluări
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Adaptive RadiotherapyDocument95 paginiAdaptive RadiotherapyGina RÎncă nu există evaluări
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- Nursing Infomatics Hospital/Critical Care ApplicationsDocument42 paginiNursing Infomatics Hospital/Critical Care ApplicationsKyla CarbonelÎncă nu există evaluări
- Guide To Dilution and Administration of Iv Medications: AcyclovirDocument29 paginiGuide To Dilution and Administration of Iv Medications: AcyclovirCiara Marjorie HannaÎncă nu există evaluări
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (345)
- White Blood Cells TugasDocument6 paginiWhite Blood Cells TugasanisaÎncă nu există evaluări
- 2.early Pregnancy and BleedingDocument79 pagini2.early Pregnancy and BleedingjosephÎncă nu există evaluări
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- Abnormal Psych CH 9 & 10 Power Pts 16Document38 paginiAbnormal Psych CH 9 & 10 Power Pts 16Natalya CespedesÎncă nu există evaluări
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Health Effects of Smoking Among Young PeopleDocument2 paginiHealth Effects of Smoking Among Young PeopleJessicaÎncă nu există evaluări
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- Presentation DH (Repaired)Document22 paginiPresentation DH (Repaired)Anmol SinghÎncă nu există evaluări
- My Own Life: by Oliver SacksDocument4 paginiMy Own Life: by Oliver SacksAmerigo VespucciÎncă nu există evaluări
- Doctors Opinion UPDATEDDocument3 paginiDoctors Opinion UPDATEDgpaul44Încă nu există evaluări
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- Disease-WPS OfficeDocument4 paginiDisease-WPS OfficeSHUBHANG SHARMAÎncă nu există evaluări
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- Hinoguin, Jocelyn Patana 1851114785Document3 paginiHinoguin, Jocelyn Patana 1851114785Paulline Joyce HinoguinÎncă nu există evaluări
- Fire Risk Assessment ScoreDocument1 paginăFire Risk Assessment ScoreYeng LimÎncă nu există evaluări
- HTAR FormularyDocument204 paginiHTAR FormularyMay TanÎncă nu există evaluări
- Airway Management and Common ConditionsDocument34 paginiAirway Management and Common Conditionsrigo montejoÎncă nu există evaluări
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- Nested Case Control StudyDocument16 paginiNested Case Control Studyqtftwkwlf100% (1)
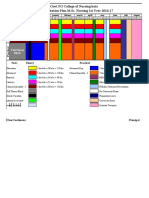
- 10.master Rotation Plan M. Sc. Nursing 1st YearDocument4 pagini10.master Rotation Plan M. Sc. Nursing 1st YearNaresh JeengarÎncă nu există evaluări
- Observation On Therapeutic Effects of Cupping Therapy For Allergic RhinitisDocument2 paginiObservation On Therapeutic Effects of Cupping Therapy For Allergic Rhinitischakir BezzahiÎncă nu există evaluări
- 8163-Article Text-29935-1-10-20110805Document3 pagini8163-Article Text-29935-1-10-20110805Wa Nur Arlin RahmadhantyÎncă nu există evaluări
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- NZMSA Guide To Graduation 2012Document40 paginiNZMSA Guide To Graduation 2012Vijaya RajÎncă nu există evaluări
- Handouts - PsychiatricDocument4 paginiHandouts - Psychiatricsendang JÎncă nu există evaluări
- Diabetic Foot UlcersDocument38 paginiDiabetic Foot UlcersRidaÎncă nu există evaluări
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)