S-ar putea să vă placă și
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- 2020 - Detecting Ethambutol Resistance in Mycobacterium Tuberculosis Isolates in China A Comparison Between Phenotypic Drug Susceptibility Testing Methods and DNA Sequencing of embABDocument7 pagini2020 - Detecting Ethambutol Resistance in Mycobacterium Tuberculosis Isolates in China A Comparison Between Phenotypic Drug Susceptibility Testing Methods and DNA Sequencing of embABNurul RifqianiÎncă nu există evaluări
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (399)
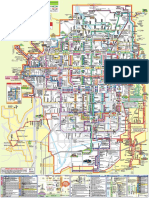
- Bus Navi 2Document1 paginăBus Navi 2Nurul RifqianiÎncă nu există evaluări
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Worsening or Development of Syringomyelia FollowingDocument6 paginiWorsening or Development of Syringomyelia FollowingNurul RifqianiÎncă nu există evaluări
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (894)
- Pathophysiology and Treatment of Neuropathic Pain AssociatedDocument9 paginiPathophysiology and Treatment of Neuropathic Pain AssociatedNurul RifqianiÎncă nu există evaluări
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Bus Navi 1Document1 paginăBus Navi 1Nurul RifqianiÎncă nu există evaluări
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Hepatolithiasis May Increase Risk of CholangiocarcinomaDocument4 paginiHepatolithiasis May Increase Risk of CholangiocarcinomaNurul RifqianiÎncă nu există evaluări
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Sy Ringo My EliaDocument13 paginiSy Ringo My EliaNurul RifqianiÎncă nu există evaluări
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Ni Hms 407962Document26 paginiNi Hms 407962Nurul RifqianiÎncă nu există evaluări
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (587)
- Review Article: Cholangiocarcinoma: Biology, Clinical Management, and Pharmacological PerspectivesDocument14 paginiReview Article: Cholangiocarcinoma: Biology, Clinical Management, and Pharmacological PerspectivesNurul RifqianiÎncă nu există evaluări
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (265)
- Cholangiocarcinoma Current Knowledge and New DevelopmentsDocument14 paginiCholangiocarcinoma Current Knowledge and New DevelopmentsNurul RifqianiÎncă nu există evaluări
- A Review of The Clinical Diagnosis and Therapy of CholangiocarcinomaDocument14 paginiA Review of The Clinical Diagnosis and Therapy of CholangiocarcinomaNurul RifqianiÎncă nu există evaluări
- Trillium Seismometer: User GuideDocument34 paginiTrillium Seismometer: User GuideDjibril Idé AlphaÎncă nu există evaluări
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- Money Laundering in Online Trading RegulationDocument8 paginiMoney Laundering in Online Trading RegulationSiti Rabiah MagfirohÎncă nu există evaluări
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (73)
- Human Rights Alert: Corrective Actions in Re: Litigation Involving Financial InstitutionsDocument3 paginiHuman Rights Alert: Corrective Actions in Re: Litigation Involving Financial InstitutionsHuman Rights Alert - NGO (RA)Încă nu există evaluări
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- AtlasConcorde NashDocument35 paginiAtlasConcorde NashMadalinaÎncă nu există evaluări
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- IQ CommandDocument6 paginiIQ CommandkuoliusÎncă nu există evaluări
- CDI-AOS-CX 10.4 Switching Portfolio Launch - Lab V4.01Document152 paginiCDI-AOS-CX 10.4 Switching Portfolio Launch - Lab V4.01Gilles DellaccioÎncă nu există evaluări
- Case Study IndieDocument6 paginiCase Study IndieDaniel YohannesÎncă nu există evaluări
- MQC Lab Manual 2021-2022-AutonomyDocument39 paginiMQC Lab Manual 2021-2022-AutonomyAniket YadavÎncă nu există evaluări
- MCQ Ch16solDocument4 paginiMCQ Ch16solandiswahlongwa870Încă nu există evaluări
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- Process Financial Transactions and Extract Interim Reports - 025735Document37 paginiProcess Financial Transactions and Extract Interim Reports - 025735l2557206Încă nu există evaluări
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2219)
- Maharashtra Auto Permit Winner ListDocument148 paginiMaharashtra Auto Permit Winner ListSadik Shaikh50% (2)
- Brochure en 2014 Web Canyon Bikes How ToDocument36 paginiBrochure en 2014 Web Canyon Bikes How ToRadivizija PortalÎncă nu există evaluări
- Dolni VestoniceDocument34 paginiDolni VestoniceOlha PodufalovaÎncă nu există evaluări
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- SOP-for RecallDocument3 paginiSOP-for RecallNilove PervezÎncă nu există evaluări
- Form 709 United States Gift Tax ReturnDocument5 paginiForm 709 United States Gift Tax ReturnBogdan PraščevićÎncă nu există evaluări
- The Smith Generator BlueprintsDocument36 paginiThe Smith Generator BlueprintsZoran AleksicÎncă nu există evaluări
- Copula and Multivariate Dependencies: Eric MarsdenDocument48 paginiCopula and Multivariate Dependencies: Eric MarsdenJeampierr Jiménez CheroÎncă nu există evaluări
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (119)
- Chapter 19 - 20 Continuous Change - Transorganizational ChangeDocument12 paginiChapter 19 - 20 Continuous Change - Transorganizational ChangeGreen AvatarÎncă nu există evaluări
- Paradigms of ManagementDocument2 paginiParadigms of ManagementLaura TicoiuÎncă nu există evaluări
- Seminar Course Report ON Food SafetyDocument25 paginiSeminar Course Report ON Food SafetyYanÎncă nu există evaluări
- CBSE Class 6 Whole Numbers WorksheetDocument2 paginiCBSE Class 6 Whole Numbers WorksheetPriyaprasad PandaÎncă nu există evaluări
- Critical Methodology Analysis: 360' Degree Feedback: Its Role in Employee DevelopmentDocument3 paginiCritical Methodology Analysis: 360' Degree Feedback: Its Role in Employee DevelopmentJatin KaushikÎncă nu există evaluări
- New Hire WorkbookDocument40 paginiNew Hire WorkbookkÎncă nu există evaluări
- Baobab MenuDocument4 paginiBaobab Menuperseverence mahlamvanaÎncă nu există evaluări
- Pulse Width ModulationDocument13 paginiPulse Width Modulationhimanshu jainÎncă nu există evaluări
- Empanelment of Architect-Consultant - Work Costing More Than 200 Lacs. (Category-B)Document6 paginiEmpanelment of Architect-Consultant - Work Costing More Than 200 Lacs. (Category-B)HARSHITRAJ KOTIYAÎncă nu există evaluări
- WindSonic GPA Manual Issue 20Document31 paginiWindSonic GPA Manual Issue 20stuartÎncă nu există evaluări
- What Is A Problem?: Method + Answer SolutionDocument17 paginiWhat Is A Problem?: Method + Answer SolutionShailaMae VillegasÎncă nu există evaluări
- Grading System The Inconvenient Use of The Computing Grades in PortalDocument5 paginiGrading System The Inconvenient Use of The Computing Grades in PortalJm WhoooÎncă nu există evaluări
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)