S-ar putea să vă placă și
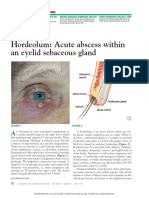
- Hordeolum: Acute Abscess Within An Eyelid Sebaceous Gland: The Clinical PictureDocument3 paginiHordeolum: Acute Abscess Within An Eyelid Sebaceous Gland: The Clinical PictureCamÎncă nu există evaluări
- Orbital and Ocular TumorsDocument13 paginiOrbital and Ocular TumorsstarlytexpressÎncă nu există evaluări
- Ophthalmology NotesDocument79 paginiOphthalmology NotesWise AmroÎncă nu există evaluări
- The Cornea PPT EditDocument38 paginiThe Cornea PPT EditRahman Setiawan100% (1)
- InfectionDocument3 paginiInfectionAndrew BonusÎncă nu există evaluări
- Special Senses 2014 - 1Document91 paginiSpecial Senses 2014 - 1Winz DolleteÎncă nu există evaluări
- Care For Patients With Alteration in Perception and CoordinationDocument12 paginiCare For Patients With Alteration in Perception and Coordinationevlujtrep9690100% (1)
- Homoeopathic Treatment of Complicated Sebaceous Cyst - A Case StudyDocument5 paginiHomoeopathic Treatment of Complicated Sebaceous Cyst - A Case StudyDr deepakÎncă nu există evaluări
- Skin Rashes in ChildrenDocument11 paginiSkin Rashes in ChildrenwiladamanikÎncă nu există evaluări
- Disorders of The Eye LidsDocument33 paginiDisorders of The Eye Lidsc/risaaq yuusuf ColoowÎncă nu există evaluări
- Blepharitis: Dr.T. Kurinchi, MsDocument39 paginiBlepharitis: Dr.T. Kurinchi, MsNailul RosyidaÎncă nu există evaluări
- M0307. Healing of Oral WoundsDocument47 paginiM0307. Healing of Oral WoundsnarmaÎncă nu există evaluări
- Male Genital DermDocument112 paginiMale Genital DermVũ CaoÎncă nu există evaluări
- Penyakit Palpebra Dan AdneksaDocument39 paginiPenyakit Palpebra Dan AdneksaayucicuÎncă nu există evaluări
- Jogi - Hordoleum KalazionDocument4 paginiJogi - Hordoleum KalazionhiÎncă nu există evaluări
- Kuliah Mata Merah, Kelainan Struktur Dan Bentuk Mata - DR NaziyaDocument47 paginiKuliah Mata Merah, Kelainan Struktur Dan Bentuk Mata - DR NaziyaFastiati RAÎncă nu există evaluări
- CORNEADocument38 paginiCORNEASamirÎncă nu există evaluări
- Abses DMDocument19 paginiAbses DMAngel MakinÎncă nu există evaluări
- Race Dermatology 2024 by DR AshishDocument29 paginiRace Dermatology 2024 by DR AshishdrshekarforyouÎncă nu există evaluări
- Internal Hordeolum. It May Point To The Skin or External Hordeolum (Stye)Document5 paginiInternal Hordeolum. It May Point To The Skin or External Hordeolum (Stye)Janella SuerteÎncă nu există evaluări
- Uveitis: Preceptor: Dr. Rahmad Syuhada, SP.M Wulandari, S.Ked 17360077Document23 paginiUveitis: Preceptor: Dr. Rahmad Syuhada, SP.M Wulandari, S.Ked 17360077widya melianitaÎncă nu există evaluări
- Ho Skin InfectionsDocument10 paginiHo Skin Infectionsnalinigobin22Încă nu există evaluări
- Disease of Lids and Lacrim Al Apparatus: The First Affiliated Hospital of Zhengzhou UniversityDocument46 paginiDisease of Lids and Lacrim Al Apparatus: The First Affiliated Hospital of Zhengzhou Universityapi-19916399Încă nu există evaluări
- Diseases of Eyelid: Prepared by DR - Sourab Kumar DasDocument66 paginiDiseases of Eyelid: Prepared by DR - Sourab Kumar Dasসপ্নে ছোয়া মনÎncă nu există evaluări
- AK Khurana - Hordoleum KalazionDocument3 paginiAK Khurana - Hordoleum KalazionhiÎncă nu există evaluări
- SCROFULODERMADocument25 paginiSCROFULODERMAFaradiba MaricarÎncă nu există evaluări
- Dry Eye DiseaseDocument8 paginiDry Eye DiseaseaÎncă nu există evaluări
- The Diagnosis and Treatment of PyodermaDocument23 paginiThe Diagnosis and Treatment of PyodermaFeby AnandaÎncă nu există evaluări
- Concept Map of CellulitisDocument8 paginiConcept Map of CellulitisReese Anne100% (1)
- PsoriasisDocument27 paginiPsoriasisNikkaDablioÎncă nu există evaluări
- Mandell, Douglas, and Bennett's Principles and Practice of Infectious Diseases, Updated Edition - Periocular Infections PDFDocument10 paginiMandell, Douglas, and Bennett's Principles and Practice of Infectious Diseases, Updated Edition - Periocular Infections PDFCarimaGhalieÎncă nu există evaluări
- High Risk School Age and AdolescentDocument6 paginiHigh Risk School Age and AdolescentRamos, Janica De VeraÎncă nu există evaluări
- CorneaDocument5 paginiCorneaMohamed GhanemÎncă nu există evaluări
- Antibiotics: Cellulitis in ChildrenDocument16 paginiAntibiotics: Cellulitis in Childrenyoona chanÎncă nu există evaluări
- OnlineMedEd Notes Dermatology 2021Document8 paginiOnlineMedEd Notes Dermatology 2021kirannhyd100% (1)
- Hordeulum, Chalazion, Pyogenic GranulomaDocument4 paginiHordeulum, Chalazion, Pyogenic Granulomaaksy100% (1)
- Draft Case 2. Acne VulgarisDocument30 paginiDraft Case 2. Acne VulgarisVirgi AhmadÎncă nu există evaluări
- Gerhard Grevers - M.D Rudolf Probst - Iro Heinrich Iro - Basic Otorhinolaryngology - A Step-By-Step Learning Guide (2018) - Libgen - LiDocument1 paginăGerhard Grevers - M.D Rudolf Probst - Iro Heinrich Iro - Basic Otorhinolaryngology - A Step-By-Step Learning Guide (2018) - Libgen - LiShai SorianoÎncă nu există evaluări
- Care For Patients With Alteration in Perception and CoordinationDocument13 paginiCare For Patients With Alteration in Perception and Coordinationevlujtrep9690Încă nu există evaluări
- Kuliah InfeksiDocument88 paginiKuliah InfeksiuupupupÎncă nu există evaluări
- Adult I Study Guide Exam 1Document23 paginiAdult I Study Guide Exam 1Christopher JamesÎncă nu există evaluări
- ConjunctivaDocument40 paginiConjunctivaSarahÎncă nu există evaluări
- Lesi Rongga Mulut Diagnosis Dan Penanganannya PDFDocument35 paginiLesi Rongga Mulut Diagnosis Dan Penanganannya PDFFhaÎncă nu există evaluări
- GS+Notes ShammaDocument225 paginiGS+Notes ShammaAisha Baniyas??Încă nu există evaluări
- Jurnal PruritusDocument4 paginiJurnal Pruritusdvunsrat agt2021Încă nu există evaluări
- Corneal Opacity ManagementDocument5 paginiCorneal Opacity ManagementAgWan Finger BillÎncă nu există evaluări
- Kelainan Kelopak (Hordeolum, Chalazion, Trichiasis, Blefaritis)Document19 paginiKelainan Kelopak (Hordeolum, Chalazion, Trichiasis, Blefaritis)Wulan NeenÎncă nu există evaluări
- Dengue Drug Study and NCPDocument22 paginiDengue Drug Study and NCPLadybelle GototosÎncă nu există evaluări
- Diseases of CorneaDocument170 paginiDiseases of CorneaLavanya MadabushiÎncă nu există evaluări
- Eye Diseases Related To Focal Dental InfectionDocument30 paginiEye Diseases Related To Focal Dental InfectionArya DananjayaÎncă nu există evaluări
- Corneea EnglishDocument57 paginiCorneea EnglishGermanyÎncă nu există evaluări
- 8.acne and LPDocument37 pagini8.acne and LPmy Lord JesusÎncă nu există evaluări
- Disease of Orbit, LacrimalDocument73 paginiDisease of Orbit, LacrimalMarshet GeteÎncă nu există evaluări
- Phase 4 Ophthalmology 2021-22Document62 paginiPhase 4 Ophthalmology 2021-22Olivia Genevieve El JassarÎncă nu există evaluări
- Eyelids, Lacrimal Apparatus and Orbit: Yonas Abraham, M.DDocument43 paginiEyelids, Lacrimal Apparatus and Orbit: Yonas Abraham, M.DTemie EshetÎncă nu există evaluări
- Orofacial Infections PDFDocument19 paginiOrofacial Infections PDFMai TÎncă nu există evaluări
- Peripheral Inflammatory Corneal Disease (Non-Infectious Keratitis) By:Mohammed SDocument66 paginiPeripheral Inflammatory Corneal Disease (Non-Infectious Keratitis) By:Mohammed SGetenet shumetÎncă nu există evaluări
- ConjungtivitisDocument86 paginiConjungtivitisIvo AfianiÎncă nu există evaluări
- Research in Uveitis and Ocular Inflammation 2011 To 2012 PDFDocument12 paginiResearch in Uveitis and Ocular Inflammation 2011 To 2012 PDFNur Rakhma AkmaliaÎncă nu există evaluări
- McAlinden Hordeolum PDFDocument3 paginiMcAlinden Hordeolum PDFNur Rakhma AkmaliaÎncă nu există evaluări
- Diagnosis and Management of Red EyeDocument8 paginiDiagnosis and Management of Red EyeNelly AstikaÎncă nu există evaluări
- McAlinden Hordeolum PDFDocument3 paginiMcAlinden Hordeolum PDFNur Rakhma AkmaliaÎncă nu există evaluări
- McAlinden Hordeolum PDFDocument3 paginiMcAlinden Hordeolum PDFNur Rakhma AkmaliaÎncă nu există evaluări
- Japan Guidelines Thyroid Storm 2016Document40 paginiJapan Guidelines Thyroid Storm 2016Irma KurniawatiÎncă nu există evaluări
- 2013 Article 3193 PDFDocument4 pagini2013 Article 3193 PDFNur Rakhma AkmaliaÎncă nu există evaluări
- Keratitis Filamentosa Pada Pasien Sjogrens Syndrome Sekunder - Sindi .SusiDocument13 paginiKeratitis Filamentosa Pada Pasien Sjogrens Syndrome Sekunder - Sindi .SusiNur Rakhma AkmaliaÎncă nu există evaluări
- Review of Intermediate UveitisDocument13 paginiReview of Intermediate UveitisNur Rakhma AkmaliaÎncă nu există evaluări
- What%27s New in Uveitis and Ocular InflammationDocument2 paginiWhat%27s New in Uveitis and Ocular InflammationNur Rakhma AkmaliaÎncă nu există evaluări
- Research in Uveitis and Ocular Inflammation 2011 To 2012 PDFDocument12 paginiResearch in Uveitis and Ocular Inflammation 2011 To 2012 PDFNur Rakhma AkmaliaÎncă nu există evaluări
- The Open Ophthalmology Journal: Editorial: Update On Glaucoma Diagnosis and ManagementDocument2 paginiThe Open Ophthalmology Journal: Editorial: Update On Glaucoma Diagnosis and ManagementNur Rakhma AkmaliaÎncă nu există evaluări
- Editorial: Update On Uveitis ManagementDocument1 paginăEditorial: Update On Uveitis ManagementNur Rakhma AkmaliaÎncă nu există evaluări
- Sss155 Slide RefraksiDocument14 paginiSss155 Slide RefraksiNur Rakhma AkmaliaÎncă nu există evaluări
- Update On Normal Tension Glaucoma: Review ArticleDocument5 paginiUpdate On Normal Tension Glaucoma: Review ArticleNur Rakhma AkmaliaÎncă nu există evaluări
- Research in Uveitis and Ocular Inflammation 2011 To 2012 PDFDocument12 paginiResearch in Uveitis and Ocular Inflammation 2011 To 2012 PDFNur Rakhma AkmaliaÎncă nu există evaluări
- Diagnosis and Management of Red EyeDocument8 paginiDiagnosis and Management of Red EyeNelly AstikaÎncă nu există evaluări
- Research in Uveitis and Ocular Inflammation 2011 To 2012 PDFDocument12 paginiResearch in Uveitis and Ocular Inflammation 2011 To 2012 PDFNur Rakhma AkmaliaÎncă nu există evaluări
- Clinical Practice Guidelines For Hypothyroidism in Adults: AACE and ATA 2012Document63 paginiClinical Practice Guidelines For Hypothyroidism in Adults: AACE and ATA 2012Nur Rakhma AkmaliaÎncă nu există evaluări
- P 137Document8 paginiP 137Nur Rakhma AkmaliaÎncă nu există evaluări
- Editorial: Update On Uveitis ManagementDocument1 paginăEditorial: Update On Uveitis ManagementNur Rakhma AkmaliaÎncă nu există evaluări
- Management Spinal Cord Injury (Sinta)Document8 paginiManagement Spinal Cord Injury (Sinta)Nur Rakhma AkmaliaÎncă nu există evaluări
- Review of Intermediate UveitisDocument13 paginiReview of Intermediate UveitisNur Rakhma AkmaliaÎncă nu există evaluări
- Jurnal Endah PDFDocument13 paginiJurnal Endah PDFNur Rakhma AkmaliaÎncă nu există evaluări
- Guidelines TBC TerbaruDocument160 paginiGuidelines TBC TerbaruSutoto MoeljadiÎncă nu există evaluări
- Update Colorectal Surgery PDFDocument9 paginiUpdate Colorectal Surgery PDFNur Rakhma AkmaliaÎncă nu există evaluări
- Tuberkulosis PDPI 2006 PDFDocument22 paginiTuberkulosis PDPI 2006 PDFNur Rakhma AkmaliaÎncă nu există evaluări
- ABC TableDocument2 paginiABC TableRosSimbulanÎncă nu există evaluări
- Update Colorectal SurgeryDocument9 paginiUpdate Colorectal SurgeryNur Rakhma AkmaliaÎncă nu există evaluări
- NERVOUS SYSTEM - pptx-2Document39 paginiNERVOUS SYSTEM - pptx-2jeffinjoffiÎncă nu există evaluări
- 2018 - The Growth and Body Composition of AnimalDocument5 pagini2018 - The Growth and Body Composition of AnimalZaheer HussainÎncă nu există evaluări
- A&P Principles of Microbiology and Human Disease (Nursing) - PowerPointDocument47 paginiA&P Principles of Microbiology and Human Disease (Nursing) - PowerPointLinsey Bowen100% (2)
- Lecture Notes - MEDICAL PARASITOLOGYDocument12 paginiLecture Notes - MEDICAL PARASITOLOGYAngelica Marzo67% (3)
- The Tangled Bank An Introduction To Evolution Second Edition Ebook PDF VersionDocument62 paginiThe Tangled Bank An Introduction To Evolution Second Edition Ebook PDF Versionwillie.getz795100% (34)
- 4) Epidemiology of Periodontal DiseasesDocument22 pagini4) Epidemiology of Periodontal Diseaseswalaa75Încă nu există evaluări
- Wonder Dogs Special Features Jordan TaylorDocument24 paginiWonder Dogs Special Features Jordan TaylorLhayka AtilloÎncă nu există evaluări
- Dairy Farmers Training ManualDocument98 paginiDairy Farmers Training ManualGrowel Agrovet Private Limited.100% (1)
- DevelopmentofocclusionDocument33 paginiDevelopmentofocclusionDeepak NarayanÎncă nu există evaluări
- 0610 m16 Ms 42Document10 pagini0610 m16 Ms 42Keshav JindalÎncă nu există evaluări
- Physiology of Muscle Contraction and Control of MovementDocument69 paginiPhysiology of Muscle Contraction and Control of MovementMakmunNawil100% (1)
- Animal Welfare Act of 1998 As AmendedDocument4 paginiAnimal Welfare Act of 1998 As AmendedRex SagauinitÎncă nu există evaluări
- Sjavs 24a270 281Document12 paginiSjavs 24a270 281Ramesh BeniwalÎncă nu există evaluări
- Zoo102 - Mammalia MetatheriaDocument37 paginiZoo102 - Mammalia MetatheriaSushmita Zen BanaagÎncă nu există evaluări
- Body Condition of Dairy Cows PDFDocument44 paginiBody Condition of Dairy Cows PDFfranky100% (1)
- LPL - PSC Rohini (DC Chowk) Shop No. 27, Ground Floor, SG Mall, Sect or - 9, DC Chowk, Rohini New Delhi - 110 DelhiDocument2 paginiLPL - PSC Rohini (DC Chowk) Shop No. 27, Ground Floor, SG Mall, Sect or - 9, DC Chowk, Rohini New Delhi - 110 DelhiSaurabh GuptaÎncă nu există evaluări
- THE INCONCEIVABLE LIFE OF QUINN Chapter SamplerDocument31 paginiTHE INCONCEIVABLE LIFE OF QUINN Chapter SamplerAbrams BooksÎncă nu există evaluări
- Axial Skeleton, ENDOSKELETON OF VERTEBRATESDocument52 paginiAxial Skeleton, ENDOSKELETON OF VERTEBRATESDave MarimonÎncă nu există evaluări
- Lec1 WildlifeDocument22 paginiLec1 WildlifeAkhshayaaÎncă nu există evaluări
- Topic Test: Oxfordaqa International Gcse Biology 9201Document26 paginiTopic Test: Oxfordaqa International Gcse Biology 9201Novanolo Christovori ZebuaÎncă nu există evaluări
- Gibco Neurobiology Protocols HandbookDocument110 paginiGibco Neurobiology Protocols HandbookIsaac Nicholas Notorio0% (1)
- كتاب اسئلة جميلDocument401 paginiكتاب اسئلة جميلMohammadSAL-Rawashdeh100% (1)
- Chapter 24. Sense Organs: ObjectivesDocument25 paginiChapter 24. Sense Organs: ObjectivesFrancisco GonzálezÎncă nu există evaluări
- Primeros Auxilios AHADocument17 paginiPrimeros Auxilios AHACarolina LópezCamperoÎncă nu există evaluări
- Malaria Control BrochureDocument2 paginiMalaria Control BrochureEkwoh Okwuchukwu EÎncă nu există evaluări
- Plr9 and Procedure For Lab Activity 9 MicparaDocument3 paginiPlr9 and Procedure For Lab Activity 9 MicparaLance sorianoÎncă nu există evaluări
- No Singkatan Nama PenyakitDocument7 paginiNo Singkatan Nama Penyakitreni riyantiÎncă nu există evaluări
- (INFEKSI) - FKUI - Nelwan Score Typhoid Fever.2016Document10 pagini(INFEKSI) - FKUI - Nelwan Score Typhoid Fever.2016Yolanda FitrianiÎncă nu există evaluări
- PuerperiumDocument85 paginiPuerperiumHema MaliniÎncă nu există evaluări
- Eco en UrgenciasDocument25 paginiEco en UrgenciasCristina Regueiro AraujoÎncă nu există evaluări
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedDe la EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedEvaluare: 5 din 5 stele5/5 (80)
- The Obesity Code: Unlocking the Secrets of Weight LossDe la EverandThe Obesity Code: Unlocking the Secrets of Weight LossEvaluare: 4 din 5 stele4/5 (6)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDDe la EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDEvaluare: 5 din 5 stele5/5 (1)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeDe la EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeEvaluare: 2 din 5 stele2/5 (1)
- The Age of Magical Overthinking: Notes on Modern IrrationalityDe la EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityEvaluare: 4 din 5 stele4/5 (26)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionDe la EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionEvaluare: 4 din 5 stele4/5 (404)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisDe la EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisEvaluare: 4.5 din 5 stele4.5/5 (42)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsDe la EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsEvaluare: 5 din 5 stele5/5 (1)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaDe la EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaEvaluare: 4.5 din 5 stele4.5/5 (266)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisDe la EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisEvaluare: 4 din 5 stele4/5 (1)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsDe la EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsÎncă nu există evaluări
- Why We Die: The New Science of Aging and the Quest for ImmortalityDe la EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityEvaluare: 4 din 5 stele4/5 (3)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryDe la EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryEvaluare: 4 din 5 stele4/5 (44)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.De la EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Evaluare: 4.5 din 5 stele4.5/5 (110)
- Gut: the new and revised Sunday Times bestsellerDe la EverandGut: the new and revised Sunday Times bestsellerEvaluare: 4 din 5 stele4/5 (392)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisDe la EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisEvaluare: 3.5 din 5 stele3.5/5 (2)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsDe la EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsEvaluare: 3.5 din 5 stele3.5/5 (3)
- The Marshmallow Test: Mastering Self-ControlDe la EverandThe Marshmallow Test: Mastering Self-ControlEvaluare: 4.5 din 5 stele4.5/5 (58)
- Dark Psychology: Learn To Influence Anyone Using Mind Control, Manipulation And Deception With Secret Techniques Of Dark Persuasion, Undetected Mind Control, Mind Games, Hypnotism And BrainwashingDe la EverandDark Psychology: Learn To Influence Anyone Using Mind Control, Manipulation And Deception With Secret Techniques Of Dark Persuasion, Undetected Mind Control, Mind Games, Hypnotism And BrainwashingEvaluare: 4 din 5 stele4/5 (1138)
- Sleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningDe la EverandSleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningEvaluare: 4 din 5 stele4/5 (3)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsDe la EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsEvaluare: 4.5 din 5 stele4.5/5 (169)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessDe la EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessEvaluare: 4.5 din 5 stele4.5/5 (328)
- A Brief History of Intelligence: Evolution, AI, and the Five Breakthroughs That Made Our BrainsDe la EverandA Brief History of Intelligence: Evolution, AI, and the Five Breakthroughs That Made Our BrainsEvaluare: 4.5 din 5 stele4.5/5 (6)