S-ar putea să vă placă și
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (73)
- Homeopathic Anti-Inflammatory Supplements: How Effective Are They?Document12 paginiHomeopathic Anti-Inflammatory Supplements: How Effective Are They?Jhe Nav100% (3)
- Antiepileptic Drugs-Good LectureDocument55 paginiAntiepileptic Drugs-Good LecturealijanmarwatÎncă nu există evaluări
- Contact Dermatitis 2015parameterDocument39 paginiContact Dermatitis 2015parameterSaniya Ilma ArifaÎncă nu există evaluări
- Isis Is A Terrorist Organization - Thank YouDocument1 paginăIsis Is A Terrorist Organization - Thank YouRishikesh ChakorÎncă nu există evaluări
- GMP - ScheduleM (GMP)Document76 paginiGMP - ScheduleM (GMP)maniyardhavalÎncă nu există evaluări
- GLP - D&C Act 1940Document48 paginiGLP - D&C Act 1940Rishikesh ChakorÎncă nu există evaluări
- Indian Patent Law - RNPDocument40 paginiIndian Patent Law - RNPRishikesh ChakorÎncă nu există evaluări
- Hatch Waxmann ActDocument5 paginiHatch Waxmann ActRishikesh ChakorÎncă nu există evaluări
- AssainmentDocument16 paginiAssainmentRishikesh ChakorÎncă nu există evaluări
- Website Material On IprDocument6 paginiWebsite Material On IprKumaran NarayananÎncă nu există evaluări
- IndexDocument1 paginăIndexRishikesh ChakorÎncă nu există evaluări
- 6 Materials and Equipments 4.8.2011Document2 pagini6 Materials and Equipments 4.8.2011Rishikesh ChakorÎncă nu există evaluări
- List of Abbrevation 4-8Document3 paginiList of Abbrevation 4-8Rishikesh ChakorÎncă nu există evaluări
- 3) Need of WorkDocument3 pagini3) Need of WorkRishikesh ChakorÎncă nu există evaluări
- USFDA A To Z DefinationDocument26 paginiUSFDA A To Z DefinationRishikesh ChakorÎncă nu există evaluări
- Index 4-8Document1 paginăIndex 4-8Rishikesh ChakorÎncă nu există evaluări
- InsertsDocument11 paginiInsertsRishikesh ChakorÎncă nu există evaluări
- Apparatus PDFDocument27 paginiApparatus PDFRishikesh ChakorÎncă nu există evaluări
- 11) ReferencesDocument15 pagini11) ReferencesRishikesh ChakorÎncă nu există evaluări
- 4) Aims & ObjectiveDocument2 pagini4) Aims & ObjectiveRishikesh ChakorÎncă nu există evaluări
- 5 Plan of Work 4.8.2011Document1 pagină5 Plan of Work 4.8.2011Rishikesh ChakorÎncă nu există evaluări
- 5 Plan of Work 4.8.2011Document1 pagină5 Plan of Work 4.8.2011Rishikesh ChakorÎncă nu există evaluări
- 5) Plan of WorkDocument2 pagini5) Plan of WorkRishikesh ChakorÎncă nu există evaluări
- 3) Need of WorkDocument3 pagini3) Need of WorkRishikesh ChakorÎncă nu există evaluări
- Materials and Instruments: 6.1. DRUG: ADAPALENE: Gift Sample From Abbott Healthcare Pvt. LTDDocument3 paginiMaterials and Instruments: 6.1. DRUG: ADAPALENE: Gift Sample From Abbott Healthcare Pvt. LTDRishikesh ChakorÎncă nu există evaluări
- 4) Aims & ObjectiveDocument2 pagini4) Aims & ObjectiveRishikesh ChakorÎncă nu există evaluări
- The Society of Hospital Pharmacists of Australia - Standards of Practice For Clinical Pharmacy - 2004Document25 paginiThe Society of Hospital Pharmacists of Australia - Standards of Practice For Clinical Pharmacy - 2004Yolita Satya Gitya UtamiÎncă nu există evaluări
- 06 Chapter 1Document47 pagini06 Chapter 1Rishikesh ChakorÎncă nu există evaluări
- Today's World: Tricia Aspinall, Anette Capel, Advanced Masterclasss CAE Workbook, Oxford University Press, 2006, P. 138Document11 paginiToday's World: Tricia Aspinall, Anette Capel, Advanced Masterclasss CAE Workbook, Oxford University Press, 2006, P. 138Mariana PopaÎncă nu există evaluări
- Make Better DecisionsDocument22 paginiMake Better DecisionsshaikhsaadahmedÎncă nu există evaluări
- AsthmaDocument2 paginiAsthmaMarya Fanta C LupuÎncă nu există evaluări
- Pivot 4a Lesson Exemplar in Mapeh 6Document7 paginiPivot 4a Lesson Exemplar in Mapeh 6Crisente BarcelonÎncă nu există evaluări
- ICICI Pru Balanced Advantage Fund - PortfolioDocument2 paginiICICI Pru Balanced Advantage Fund - PortfolioSunil ChaudharyÎncă nu există evaluări
- Antidepressant Efficacy For Depression in Children and Adolescents: Industry-And NIMH-Funded StudiesDocument8 paginiAntidepressant Efficacy For Depression in Children and Adolescents: Industry-And NIMH-Funded StudiesResidentes dieciocho veintidósÎncă nu există evaluări
- 079 BorseDocument9 pagini079 BorsepuriwatiÎncă nu există evaluări
- Data Bu ShellaDocument114 paginiData Bu Shellaruri nur indahÎncă nu există evaluări
- Permethrin TechnicalDocument5 paginiPermethrin TechnicalHuyen NguyenÎncă nu există evaluări
- The Efficacy of Medicinal Leeches in Plastic and Reconstructive Surgery - A Systematic Review of 277 Reported Clinical Cases-2Document11 paginiThe Efficacy of Medicinal Leeches in Plastic and Reconstructive Surgery - A Systematic Review of 277 Reported Clinical Cases-2Wara Samsarga GedeÎncă nu există evaluări
- Alims - Approved Terminology - Routes and Methods of Administration - October 2014Document2 paginiAlims - Approved Terminology - Routes and Methods of Administration - October 2014Katarina R.M.Încă nu există evaluări
- Pharmacological Interactions of VasoconstrictorsDocument8 paginiPharmacological Interactions of VasoconstrictorsValeska Farina EspinosaÎncă nu există evaluări
- MerckDocument14 paginiMerckShruthi RÎncă nu există evaluări
- Chapter 4: Company Profile 4.1 HistoryDocument5 paginiChapter 4: Company Profile 4.1 HistoryshawnratulÎncă nu există evaluări
- By:-Devang Gangwani and Ashish Juriani - Final Year Bpharm (2018)Document20 paginiBy:-Devang Gangwani and Ashish Juriani - Final Year Bpharm (2018)Devang GangwaniÎncă nu există evaluări
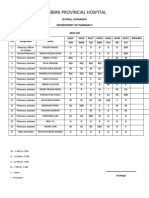
- Lumbini Provincial Hospital: Department of PharmacyDocument2 paginiLumbini Provincial Hospital: Department of PharmacyImdadHussainOPositiveÎncă nu există evaluări
- Lupin Receives Approval For Acotiamide Tablets To Treat Functional Dyspepsia (Company Update)Document3 paginiLupin Receives Approval For Acotiamide Tablets To Treat Functional Dyspepsia (Company Update)Shyam SunderÎncă nu există evaluări
- Pharmaceutics Is The Discipline of Pharmacy That Deals With The Process of Turning ADocument6 paginiPharmaceutics Is The Discipline of Pharmacy That Deals With The Process of Turning ANGMC Clinical TrialÎncă nu există evaluări
- The 6th International Conference On The History of Chemistry PDFDocument714 paginiThe 6th International Conference On The History of Chemistry PDFJose Belisar100% (2)
- Duphalac Bristol PediaFlyerDocument2 paginiDuphalac Bristol PediaFlyerNikola StojsicÎncă nu există evaluări
- Universidad Del Istmo Facultad de Ciencias Económicas y Empresariales "MBO" Talento HumanoDocument5 paginiUniversidad Del Istmo Facultad de Ciencias Económicas y Empresariales "MBO" Talento HumanoluispradoarevaloÎncă nu există evaluări
- Glucose Metformin Thiazolidinedione Pioglitazone Rosiglitazone GlucoseDocument2 paginiGlucose Metformin Thiazolidinedione Pioglitazone Rosiglitazone GlucoseDarshan MoreÎncă nu există evaluări
- Adi CholDocument4 paginiAdi CholIqbal MaulanaÎncă nu există evaluări
- Manual Dispensing (Lengkap)Document14 paginiManual Dispensing (Lengkap)zayÎncă nu există evaluări
- PHARMA 1.06-Laboratory ConferenceDocument7 paginiPHARMA 1.06-Laboratory ConferenceHayleyvanadiumÎncă nu există evaluări
- Amoxicillin 3 X 1Document1 paginăAmoxicillin 3 X 1MeilindaLaurensiaFebrihiantoÎncă nu există evaluări
- Bpharm Sem 6 Quality Assurance Ques PaperDocument3 paginiBpharm Sem 6 Quality Assurance Ques PaperNavam KumarÎncă nu există evaluări