S-ar putea să vă placă și
- Michael J McCammon - The Power of Herbal Medicine, Iridology and Nutrition PDFDocument161 paginiMichael J McCammon - The Power of Herbal Medicine, Iridology and Nutrition PDFMoga Razvan100% (3)
- HEART FAILURE-WilliamDec (2005) PDFDocument602 paginiHEART FAILURE-WilliamDec (2005) PDFChintya Fidelia MontangÎncă nu există evaluări
- Understanding Chronic Kidney Disease: A guide for the non-specialistDe la EverandUnderstanding Chronic Kidney Disease: A guide for the non-specialistEvaluare: 4 din 5 stele4/5 (3)
- Evidence-Based NephrologyDe la EverandEvidence-Based NephrologyDonald A. Molony, M.D.Încă nu există evaluări
- Early Chronic Kidney DiseaseDocument12 paginiEarly Chronic Kidney DiseaseDirga Rasyidin L100% (1)
- Castle Connolly Graduate Board Review SeriesDocument31 paginiCastle Connolly Graduate Board Review SeriesCCGMPÎncă nu există evaluări
- Handout1 - Normal Changes of AgingDocument3 paginiHandout1 - Normal Changes of Agingpissednachos0123Încă nu există evaluări
- NMCN Updated Past Question - 2012-2019-1Document37 paginiNMCN Updated Past Question - 2012-2019-1Chinaemerem100% (1)
- General Principles of Toxicology-1Document37 paginiGeneral Principles of Toxicology-1Musa yohanaÎncă nu există evaluări
- Chronickidneydisease: Cornelia Charles,, Allison H. FerrisDocument11 paginiChronickidneydisease: Cornelia Charles,, Allison H. FerrisDiahÎncă nu există evaluări
- CKD PDFDocument6 paginiCKD PDFmkafabillahÎncă nu există evaluări
- Reviews: Early Detection of CKD: The Benefits, Limitations and Effects On PrognosisDocument12 paginiReviews: Early Detection of CKD: The Benefits, Limitations and Effects On Prognosisanderson roberto oliveira de sousaÎncă nu există evaluări
- Definition and Classification of Kidney Diseases: EditorialDocument3 paginiDefinition and Classification of Kidney Diseases: EditorialdianaÎncă nu există evaluări
- Chronic Kidney Disease: SeminarDocument16 paginiChronic Kidney Disease: SeminarMichael Meng100% (1)
- Epidemiology of Chronic Kidney Disease Among Older Adults: A Focus On The Oldest OldDocument8 paginiEpidemiology of Chronic Kidney Disease Among Older Adults: A Focus On The Oldest Oldkhangha.ptÎncă nu există evaluări
- Pathophysiology and Classification of Kidney DiseasesDocument10 paginiPathophysiology and Classification of Kidney DiseasesmedicalÎncă nu există evaluări
- Introduction The Case For Updating and Co - 2013 - Kidney International SupplemDocument4 paginiIntroduction The Case For Updating and Co - 2013 - Kidney International SupplemwardaninurindahÎncă nu există evaluări
- HP Mar03 ChronicDocument6 paginiHP Mar03 ChronicAnonymous MJkYnuÎncă nu există evaluări
- Definition and Staging of Chronic Kidney Disease in Adults - UpToDateDocument37 paginiDefinition and Staging of Chronic Kidney Disease in Adults - UpToDatedarleyÎncă nu există evaluări
- Guidelines On Chronic Kidney Disease: (NKF K/Doqi)Document32 paginiGuidelines On Chronic Kidney Disease: (NKF K/Doqi)Laura PutriÎncă nu există evaluări
- BMJ 2022 074216.fullDocument20 paginiBMJ 2022 074216.fullArmando OrtegaÎncă nu există evaluări
- Approach To The Detection and Management of Chronic Kidney DiseaseDocument8 paginiApproach To The Detection and Management of Chronic Kidney Diseaseapi-301730880Încă nu există evaluări
- BM 27 153Document24 paginiBM 27 153Imam albanjariÎncă nu există evaluări
- CKD in Adults - UpToDateDocument54 paginiCKD in Adults - UpToDateNada AhmedÎncă nu există evaluări
- Chronic Kidney Disease20190605 98952 Kssgx8 With Cover Page v2Document16 paginiChronic Kidney Disease20190605 98952 Kssgx8 With Cover Page v2Melly SyafridaÎncă nu există evaluări
- Conservative Management of Chronic Renal Failure: Contemporary IssueDocument6 paginiConservative Management of Chronic Renal Failure: Contemporary IssueInes TerraheÎncă nu există evaluări
- GFR and Albuminuria Level in Acute and Chronic Kidney DiseaseDocument9 paginiGFR and Albuminuria Level in Acute and Chronic Kidney DiseaseLoreto FernandezÎncă nu există evaluări
- Chronic Kidney Disease in Adults - Assessment and ManagementDocument5 paginiChronic Kidney Disease in Adults - Assessment and ManagementAnahí Cortés HerreraÎncă nu există evaluări
- Part 9. Approach To Chronic Kidney Disease Using These GuidelinesDocument8 paginiPart 9. Approach To Chronic Kidney Disease Using These GuidelinesSudjarwo AntonÎncă nu există evaluări
- Epidemiology and Causes of Chronic Kidney Disease: What's New?Document4 paginiEpidemiology and Causes of Chronic Kidney Disease: What's New?Ika auliaÎncă nu există evaluări
- Seminar: Angela C Webster, Evi V Nagler, Rachael L Morton, Philip MassonDocument15 paginiSeminar: Angela C Webster, Evi V Nagler, Rachael L Morton, Philip MassonMaría José GalvisÎncă nu există evaluări
- 2022 NEJM Uses of GFR and Albuminuria LevelDocument9 pagini2022 NEJM Uses of GFR and Albuminuria LevelPeter Albeiro Falla CortesÎncă nu există evaluări
- KDIGO Improving CKD Quality of Care - Scope of Work - FinalDocument10 paginiKDIGO Improving CKD Quality of Care - Scope of Work - FinalGEORGINA NIEVES CHOQUETICLLAÎncă nu există evaluări
- BMJ m2687 FullDocument15 paginiBMJ m2687 FullhuevalicoÎncă nu există evaluări
- 546 FullDocument3 pagini546 FullAndreea GheorghiuÎncă nu există evaluări
- Nej MR A 2201153Document9 paginiNej MR A 2201153LETICIA CRISTINO FRANCISCOÎncă nu există evaluări
- Inbound 627074868857946511Document55 paginiInbound 627074868857946511Novelyn OlidanÎncă nu există evaluări
- Hepatorenal Syndrome: Pathophysiology, Diagnosis, and ManagementDocument15 paginiHepatorenal Syndrome: Pathophysiology, Diagnosis, and ManagementAndreina AcevedoÎncă nu există evaluări
- p4 Class g1.htmDocument14 paginip4 Class g1.htmIrara RaÎncă nu există evaluări
- Hepatorenal Syndrome Pathophysiology, Diag-Nosis, and ManagementDocument15 paginiHepatorenal Syndrome Pathophysiology, Diag-Nosis, and Managementwinny kartikaÎncă nu există evaluări
- Anemia: Chronic Kidney DiseaseDocument12 paginiAnemia: Chronic Kidney DiseasetyasÎncă nu există evaluări
- Chronic Kidney Disease in Primary Care: Duaine D. Murphree, MD, and Sarah M. Thelen, MDDocument11 paginiChronic Kidney Disease in Primary Care: Duaine D. Murphree, MD, and Sarah M. Thelen, MDMawarÎncă nu există evaluări
- A Role For SGLT 2 Inhibitors in Treating Non Diabetic Chronic Kidney DiseaseDocument21 paginiA Role For SGLT 2 Inhibitors in Treating Non Diabetic Chronic Kidney DiseaseCarlos Martinez SalgadoÎncă nu există evaluări
- Kidneydiseaseandthe Nexusofchronickidney DiseaseandacutekidneyinjuryDocument33 paginiKidneydiseaseandthe Nexusofchronickidney DiseaseandacutekidneyinjuryMardauc AnaidÎncă nu există evaluări
- Medifocus Dec 2012Document67 paginiMedifocus Dec 2012Pushpanjali Crosslay HospitalÎncă nu există evaluări
- Clinical Practice Guidelines On Hypertension and Antihypertensive Agents in Chronic Kidney Disease (CKD)Document9 paginiClinical Practice Guidelines On Hypertension and Antihypertensive Agents in Chronic Kidney Disease (CKD)Dewi Sekar AyuÎncă nu există evaluări
- Chronic Kidney Disease:: The Canary in The Coal MineDocument13 paginiChronic Kidney Disease:: The Canary in The Coal MinedhearawrsÎncă nu există evaluări
- 22-12 - Chronic Kidney DiseaseDocument19 pagini22-12 - Chronic Kidney DiseaseSergio VasquezÎncă nu există evaluări
- Progress and Epidemology of The Chronic Renal FailureDocument18 paginiProgress and Epidemology of The Chronic Renal Failuremanfel_26Încă nu există evaluări
- Definition and Staging of Chronic Kidney Disease in Adults - UpToDateDocument1 paginăDefinition and Staging of Chronic Kidney Disease in Adults - UpToDateLauraÎncă nu există evaluări
- Nej M ArticleDocument9 paginiNej M Articlelakshminivas PingaliÎncă nu există evaluări
- Chronic Kidney Disease in Children: Clinical Manifestations and EvaluationDocument30 paginiChronic Kidney Disease in Children: Clinical Manifestations and EvaluationPaula BecerraÎncă nu există evaluări
- Chronic Kidney Disease: Identification and Management in Primary CareDocument12 paginiChronic Kidney Disease: Identification and Management in Primary CareLiri AndiyaniÎncă nu există evaluări
- Chronic Kidney Disease: Rizki Aliana AgustinaDocument85 paginiChronic Kidney Disease: Rizki Aliana AgustinaRofi IrmanÎncă nu există evaluări
- Chronic Kidney DiseaseDocument42 paginiChronic Kidney DiseaseLeta GemechuÎncă nu există evaluări
- Epidemiology of Chronic Kidney Disease An U - 2022 - Kidney International SupplDocument5 paginiEpidemiology of Chronic Kidney Disease An U - 2022 - Kidney International SupplSol anonimoÎncă nu există evaluări
- Managing Chronic Kidney Disease PrimaryDocument18 paginiManaging Chronic Kidney Disease Primaryhusnaforever100% (1)
- Jurding CKD Edit-1Document20 paginiJurding CKD Edit-1Asmaul HabibiÎncă nu există evaluări
- 2 Penyakit Ginjal Kronik - Diagnosis Dan Indikasi Terapi Pengganti GinjalDocument49 pagini2 Penyakit Ginjal Kronik - Diagnosis Dan Indikasi Terapi Pengganti Ginjalmillah mahfudhoh100% (1)
- Diabetic Kidney Disease ManagementDocument16 paginiDiabetic Kidney Disease Managementcecilia zavalaÎncă nu există evaluări
- KDIGO Conclusiones EjecutivasDocument22 paginiKDIGO Conclusiones EjecutivasJuan DavidÎncă nu există evaluări
- CPG Management of Chronic Kidney Disease in Adults June 2011Document47 paginiCPG Management of Chronic Kidney Disease in Adults June 2011Kokoland KukusÎncă nu există evaluări
- Non-Steroidal Mra DKD PotassiumDocument10 paginiNon-Steroidal Mra DKD Potassiumlakshminivas PingaliÎncă nu există evaluări
- Restoring Chronic Kidney Disease : Restoring, Preserving, and Improving CKD to Avoid DialysisDe la EverandRestoring Chronic Kidney Disease : Restoring, Preserving, and Improving CKD to Avoid DialysisÎncă nu există evaluări
- Tukak GasterDocument11 paginiTukak GasterAndrie WigunaÎncă nu există evaluări
- ANEMIA Pada Penyakit KronikDocument14 paginiANEMIA Pada Penyakit KronikAndrie WigunaÎncă nu există evaluări
- Obesitas Pada Anak: DR - Sri S.Nasar, Spa (K)Document27 paginiObesitas Pada Anak: DR - Sri S.Nasar, Spa (K)Andrie WigunaÎncă nu există evaluări
- Efek Statin Dalam Menurunkan Angka Kejadian Penyakit KardiovaskularDocument6 paginiEfek Statin Dalam Menurunkan Angka Kejadian Penyakit KardiovaskularAndrie WigunaÎncă nu există evaluări
- Antiplateletdrugs 150203231404 Conversion Gate01 PDFDocument67 paginiAntiplateletdrugs 150203231404 Conversion Gate01 PDFAndrie WigunaÎncă nu există evaluări
- Hershman2018 PDFDocument10 paginiHershman2018 PDFAndrie WigunaÎncă nu există evaluări
- PCR DNA MetodeDocument11 paginiPCR DNA MetodeAndrie WigunaÎncă nu există evaluări
- PAD Guideline AHA-ACC 2016Document23 paginiPAD Guideline AHA-ACC 2016Andrie WigunaÎncă nu există evaluări
- Nosocomial Pneumonia in AdultsDocument28 paginiNosocomial Pneumonia in AdultsAndrie WigunaÎncă nu există evaluări
- DIVERTIKULOSISDocument28 paginiDIVERTIKULOSISAndrie WigunaÎncă nu există evaluări
- NAFLD-dr. Masrul KuliahDocument103 paginiNAFLD-dr. Masrul KuliahAndrie WigunaÎncă nu există evaluări
- Plasmodium Malariae Infection in An Asymptomatic 74-Year-OldDocument6 paginiPlasmodium Malariae Infection in An Asymptomatic 74-Year-OldAndrie WigunaÎncă nu există evaluări
- Responding To Organ Failure in HIV-Infected Patients: Volume 348:2279-2281 June 5, 2003 Number 23Document4 paginiResponding To Organ Failure in HIV-Infected Patients: Volume 348:2279-2281 June 5, 2003 Number 23Andrie WigunaÎncă nu există evaluări
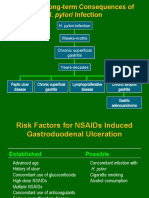
- H. Pylori Infection: Potential Long-Term Consequences ofDocument30 paginiH. Pylori Infection: Potential Long-Term Consequences ofAndrie WigunaÎncă nu există evaluări
- H. Pylori Infection: Potential Long-Term Consequences ofDocument30 paginiH. Pylori Infection: Potential Long-Term Consequences ofAndrie WigunaÎncă nu există evaluări
- Standard Operating Procedure (SOP) For On-Call Emergency Out of Hours Haemodialysis For Renal PatientsDocument23 paginiStandard Operating Procedure (SOP) For On-Call Emergency Out of Hours Haemodialysis For Renal PatientsShahriar MohammodÎncă nu există evaluări
- Diagnosis of Secondary Hypertension: An Age-Based Approach: Anthony J. Viera, MD, MPH, and Dana M. Neutze, MD, PHDDocument8 paginiDiagnosis of Secondary Hypertension: An Age-Based Approach: Anthony J. Viera, MD, MPH, and Dana M. Neutze, MD, PHDmiguel ángelÎncă nu există evaluări
- Comp ReviewDocument99 paginiComp ReviewTHAO DANGÎncă nu există evaluări
- Aku - To PrintDocument23 paginiAku - To PrintMc Crister SilangÎncă nu există evaluări
- A Rare Complication of Pauci-Immune Crescentic Glomerulonephritis in A Child: QuestionsDocument2 paginiA Rare Complication of Pauci-Immune Crescentic Glomerulonephritis in A Child: QuestionsadiÎncă nu există evaluări
- Therapeutic Plasma Exchange (TPE) : Colm Magee, MD, MPH, MRCPIDocument23 paginiTherapeutic Plasma Exchange (TPE) : Colm Magee, MD, MPH, MRCPIsigitÎncă nu există evaluări
- The Excretory System in The HumanDocument48 paginiThe Excretory System in The Humanapi-266618926Încă nu există evaluări
- Acute Nephritis SyndromeDocument39 paginiAcute Nephritis SyndromeamlymarsÎncă nu există evaluări
- Calcium MetabolismDocument28 paginiCalcium MetabolismAhmedkhaed100% (1)
- The Urinary System Overview of Kidney FunctionsDocument9 paginiThe Urinary System Overview of Kidney FunctionsLALRINTLUANGI CHHAKCHHUAKÎncă nu există evaluări
- Science 10 Prep1 Key AnswerDocument16 paginiScience 10 Prep1 Key AnswerchandanÎncă nu există evaluări
- DialysisDocument18 paginiDialysissrinithiÎncă nu există evaluări
- Diuretics and Drugs Affecting Renal Function, Water, and Electrolyte MetabolismDocument4 paginiDiuretics and Drugs Affecting Renal Function, Water, and Electrolyte MetabolismWaqar HassanÎncă nu există evaluări
- Urinalysis ChecklistDocument7 paginiUrinalysis ChecklistLana LocoÎncă nu există evaluări
- Acute Kidney Injury: Mark BevanDocument42 paginiAcute Kidney Injury: Mark BevannasimhsÎncă nu există evaluări
- Elementary Anatomy (Q-Bank 2020)Document22 paginiElementary Anatomy (Q-Bank 2020)Muhammad AdnanÎncă nu există evaluări
- Physical Changes With Aging - Geriatrics - MSD Manual Professional Edition PDFDocument5 paginiPhysical Changes With Aging - Geriatrics - MSD Manual Professional Edition PDFnamumbiÎncă nu există evaluări
- Kidney Best FoodsDocument4 paginiKidney Best FoodsDrake SuyatÎncă nu există evaluări
- EHRASurvey ManagementofAFinCKDPatients FinalManuscriptDocument10 paginiEHRASurvey ManagementofAFinCKDPatients FinalManuscriptLabontu IustinaÎncă nu există evaluări
- CASE STUDY - Community Acquired Pneumonia With Pleural Effusion & UTIDocument73 paginiCASE STUDY - Community Acquired Pneumonia With Pleural Effusion & UTIFrancis AdrianÎncă nu există evaluări
- Prosound 4000Sv: Specifications Diagnostic Ultrasound SystemDocument12 paginiProsound 4000Sv: Specifications Diagnostic Ultrasound SystemGeomar J PintoÎncă nu există evaluări
- Test Bank For Nursing A Concept Based Approach To Learning Volume 1 Nccleb DownloadDocument18 paginiTest Bank For Nursing A Concept Based Approach To Learning Volume 1 Nccleb Downloadjeremywang14102002mck100% (18)
- Wild Animal NecropsyDocument28 paginiWild Animal NecropsyJelena Jeca100% (1)
- ZOO 4733 - Exam 2 ReviewDocument25 paginiZOO 4733 - Exam 2 ReviewDaniel PóoÎncă nu există evaluări
- Chapter 26: Introduction To The Urinary SystemDocument37 paginiChapter 26: Introduction To The Urinary Systemmaatela7sasÎncă nu există evaluări
- Grade 10 12 Biology Notes ExcretionDocument13 paginiGrade 10 12 Biology Notes ExcretionNathan mwapeÎncă nu există evaluări