Documente Academic
Documente Profesional
Documente Cultură
Spectral Analysis of BP-Hypertension 1995
Încărcat de
Barış Yaradanakul0 evaluări0% au considerat acest document util (0 voturi)
1 vizualizări11 paginispectral analysis
Drepturi de autor
© © All Rights Reserved
Formate disponibile
PDF sau citiți online pe Scribd
Partajați acest document
Partajați sau inserați document
Vi se pare util acest document?
Este necorespunzător acest conținut?
Raportați acest documentspectral analysis
Drepturi de autor:
© All Rights Reserved
Formate disponibile
Descărcați ca PDF sau citiți online pe Scribd
0 evaluări0% au considerat acest document util (0 voturi)
1 vizualizări11 paginiSpectral Analysis of BP-Hypertension 1995
Încărcat de
Barış Yaradanakulspectral analysis
Drepturi de autor:
© All Rights Reserved
Formate disponibile
Descărcați ca PDF sau citiți online pe Scribd
Sunteți pe pagina 1din 11
1276
Spectral Analysis of Blood Pressure and
Heart Rate Variability in
Evaluating Cardiovascular Regulation
A Critical Appraisal
Gianfranco P:
Abstract Blood pressure variability includes shythmic and
‘nonrhythmic fluctuations that, with the use of spectral analysis,
appear as clear peaks or broadband power, respectively. This
review offers concise and critical description of the spectral
methods most commonly used (fast Fourier transform versus
utoregressive modeling, time-varying versus broadband spec
teal analysis) and an evaiuation of theie advantages and disad-
‘vantages. It also provides insight into the problems that stil
alec the physiological and clinical interpretations of dat
provided by spectral analysis of blood pressure and heart ra
variability. In particular, the assessment of blood pressure and
Ineatt rate spectra aimed at providing indexes af autonomic
he regulation of blood pressure (BP) is tradition-
ally described in terms of homeostasis." This
word comes from the Greek homeo (similar)
and stasis (steady) and indicates that BP, although being
continuously perturbed by external stimulations, always
displays the tendency to come back toward a reference
set point. This dynamic behavior of BP implies thi
attention should be directed not only to the average BP
valuc, which can be regarded as the reference set point,
but also to the BP and cardiovascular fluctuations oc
‘curring around this average. Data from a variety of
sources indicate that these fluctuations are indeed much
‘more than undesirable noise. On the contrary, they
esent a rich source of information that can provide
ight into the mechanisms of cardiovas-
cular control.** Cardiovascular fluctuations ean be stud
ied through beat-to-beat BP and heart rate (HR) mon-
itoring and calculation of the variance (or standard
deviation) of their average values Recently, how-
ever, frequency domain analysis has also been used to
subdivide the variability of BP and HR into different
Recvived September 8, 1994; fist deckion October 25, 1994
seibion accepted February 16,1995
From the Istituto Scientfico Ospedale §. Luca, Centro Auxo
logico Italiano, Milano (G-P.,G.ML), Medicina Interna I. Ospedale
S. Gerardo, Monza and Universita di Milano (G.P. G.M.) (lta.
Children’s Hospital, Department of Cardiology, Havant Medica
School, Boston (PS); Massachussetts Institute of Technolo,
Health Sciences and ‘Technology, Cambridge (.PS.), Mass. ad
LARG, Centro di Bioingegneria, Fondazione Pro Juventute, Mi-
lao, italy (M. Di R),
Correspondence to Gianfranco Parat, MD, Cento di Fisiologia
linia © Ipertensions, Ospedale Maggiore and. Universit
Milano, va F Stora,
ati, J. Philip Saul, Marco Di Rienzo, Giuseppe Mancia
cardiovascular modulation is discussed. Evidence is given that
multivariate models—which allow evalvation of the inte
ons between changes in blood pressure, heart rate, and other
biological signals (uch as respiratory activity) in the time or
frequency domains—offer 4 more comprehensive approach 10
the assessment of cardiovascular regulation than that repre
sented by the separate analysis of fictuations in blood pressure
fr heatt rate only. ypertension, 1995;25:1276-1286,)
Key Words © blood pressure « heart rate * autonomic
nervous system © hypertension, essential * sequence
analysis
frequency components and to quantify the variance or
“power” at cach specific frequency." A wide variety of
algorithms and models have been proposed in this
context to study spontancous cardiovascular variability
and to characterize the relation between the changes in
HR, arterial BP, and respiration, However, the optimal
‘methods for extracting such information and the most
appropriate interpretations of the results obtained are
still matters of considerable debate." This article will
focus on these issues.
Rhythmic and Nonrhythmic Changes in
BP and HR
Rhythmic BP and HR oscillations related to respira-
tory activity were first deseribed by Hales" and: von
Haller," and their observations were confirmed by Lud-
wig 80 years later.* After a few decades, Mayer reported
that BP also oscillates at frequencies slower than the
respiratory rhythm, suggesting that these oscillations are
related to vasomotor activity."©"* More recently, techno-
logical progress in the field of data collection and
analysis HR recording, availability
of low-cost eo gorithms for data process-
ing, etc) has led to more sophisticated approaches 10
rhythmic circulatory phenomena and to their more
frequent investigation by power spectrum analysis, Orig
inally, three BP and HR rhythmic oscillations were
identified, all with a period shorter than 1 minute and
with the appearance in the spectrum as individual peaks
(Fig 14). These peaks reflect (1) oscillations with
Frequency around 0.2 to 0.4 Hz, a frequency similar to
that of normal respiratory activity, defined as high-
frequency (HF): ions with frequency of
approximately 0.1 Hz, defined as mid-frequency (MF)
Parati ct al Cardiovascular Control and Spectral Analysis 1277
Es
Tine(ninowe) Frege er
B ‘Time Series. ‘Spectre.
eee
is! z
ae
Fro 1. Pots show respiratory and heart rate time series (ot)
and spectra (ight) for one subject with “peaky" heart rate
‘spectra (A) and one with broadband heart rate spectra (2).
and corresponding in the case of BP to the classic Mayer
‘waves; and (3) oscillations with a frequency between 01.02
and 0.07 Hz, defined as low-frequency (LF) and pro
bly related to a variety of cardiorespiratory phenomena
and mechanisms." Subsequent studies, however, have
made it clear that the amplitude and frequency of the
above oscillations are by no means constant but vary a5
4 funtion of different behavioral conditions. This is the
tse for the 0.3-Hz (HF) and 0.1-Hz (MF) oscillations. It
‘even more often the case for the 002 to 0.07-Hz
oscillations (LE), which explains why investigators base
1 their analysis on peak detection models (see below)
usually disregard these fluctuations and consider only
two major components in the spectrum, around 0.1 and
03 Ha, defined as HF and LF, respectively
Regardless of whether the spectrum is subdivided into
two oF three components, an important issue is whether
power special analysis should exclusively focus on spec-
tral peaks. The peak detection approach is supported by
4a number of investigators who believe that a peak may
fellect a specific mechanism of cardiovascular control
that can thus be quantitatively assessed by the power or
area of the peak. However, other observations suggest
that (1) a peak may originate from more than a single
cardiovascular control mechanism, and (2) a. single
cardiovascular eontrol mechanism ‘may contribute. to
different. peaks.*22* In addition, recent studies have
shown that BP and HR variability includes not only
rhythmic oscillations but also nonthythmic fluctuations
that appear in the spectrum not as clearly defined peaks
but as powers spread over a broad frequency region (Fig,
1B). It is now clear that these nonrhythmic fluctuations
are also relevant to cardiovascular control mechanisms,
10"
10!
10
10
10 107 107 10" 1
Hz
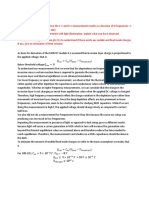
Fic 2. Plot shows broadband systolic blood pressure spectra
‘blaine from a fee-moving cat inthe intact cancion (dark lino)
f’and 3 weeks after sinoaortc denervation (SAD, light in). Stood
pressure was continuously recorded for 3 hours by means of an
intra-arterial catheter (abdominal aorta Inarted through a fem-
fra ator). Systolic pressure spectral components ranging from
Approximately 0.5 to 0.0001 Hz are considered. (Modified from
Di Fenzo et al by permission)
As an example, in unanesthetized cats under continuous
BP and HR monitoring, removal of baroreceptor re-
straint of sympathetic activity by sinoaortic denervation
is accompanied by systematic changes in nonpeaked BP
and HIR powers in several frequency regions® (Fig 2)
Furthermore, in normotensive and hypertensive sul
jects, nonpeaked BP and HR powers are modified in
systematic fashion by a condition of reduced sympathetic
and inereased vagal activity such as sleep252" Thus,
consideration of broadband powers rather than peaks
only may offer a broader description of cardiovascular
regulation,
Fast Fourier Transform Versus
Autoregressive Methods
‘The methods most commonly used for spectral analy~
sis are based on (1) the discrete Fourier transform,
‘usually implemented on the computeras the fast Fourier
* and (2) autoregressive (AR) model-
ing.!22°° The spectrum resulting from the FFT is de-
rived from all the data present in the recorded sigy
it includes the entire signal variance, regardless. of
whether its frequency components apy specific
spectral peaks or as nonpeaked broadband powers. In
contrast, with the AR procedure, the raw data are used
to identify a bestfiting model from which the final
spectrum, consisting of the DC component and a vai
able number of peaks, is derived. The components of the
signal not fitting the model are treated as noise and
partially or totally removed,!222" The above consid:
ations identify the most important dillerences between
the two methods (Fig 3) and their advantages and
‘ages in different conditions. When attention is
focused only on BP or HR rhythmic fluctuations driven
by a fixed-rate oscillator, AR methods are suitable
‘because of their ability to identify the central frequency
Of the oscillation in an analytic way. Furthermore, the
‘AR approach is particularly appropriate when the num.
1278 Hypertension Vol 25, No 6 June 1995
as.
Fic 3, Plots show the same heart rate spectra of Fig 1A ight)
and Fig 1B (of) obtained by means of diferent analysis moth-
‘ods. A, Data are plotted with an unsmoothed fast Fourier
transform (FFT) algorithm; B, data are plotted with an autore-
‘gressive (AR) model, the order (=19) of which was determined
by Akaiko entra: C, data are plotted with an FFT algorithm
smoothed with a Gaussian window and appear lke those
‘obtained with the AR model having an order of 13 (8); D, data are
plottad with an AR model with 3 high order (=30) and appear ike
{hose obtained with the unsmoothed FFT algorthm (A).
ber of samples available for the analysis is low, because
the Frequency resolution of the AR-derived spectrum is
not as dependent as the FFT method on the length of
the recording. On the other hand, when the analysis is
focused on broadband powers, the AR’ method suitably
describes the spectrum only if an appropriately high
model order is used. Unfortunately, the criteria to
automaticaly determine the model order usually lead to
seleetion of am order that tends to be tendentally love
than that necessary to describe broadband spectra.
Thus, the order so defined may need to be empirically
corrected on the basis of the investigator's experts
Under these conditions, the FFT method may be pref-
erable. It should be emphasized that in several condi-
tions, the results obtained by the FFT and AR methods
may be very lose to each other. This occurs when (I) the
‘AR model order approaches the number of data points
‘or (2) the FFT-derived speetrum is used with method
ological manipulation (eg, the Blackman-Tukey method
‘and a prewindowing and smoothing of the autocorrela-
tion function?”
Short- Versus Long-Lasting BP and
HR Recordings
Most studies on spectral analysis of BP and HR
variability make use of data segments 3 to 5 minutes long.
derived from recordings obtained under standardized
laboratory conditions after removal of possible artifacts
(an issue briefly dealt with in Appendix A). This pro-
vides reliable results when spectral components with
periods shorter than 1 minute are being considered,
regardless of whether the subject has a low or high basal
HR. On the other hand, such a spectral analysis cannot
be appropriately performed if the recording segments
are shorter than 3 minutes (LPS. unpublished data,
1994) unless the analysis focuses on components with
frequencies equal to or greater than 0.1 Hz only. In the
latter case, even a window of 1 minute in length may
suffice, although in a bradycardic subject this would
result in a low number of points available for the analysis
and thus in a crtieal reduction of the frequency resolu-
tion of the spectral estimate if the FFT method is used.
ata collected in laboratory conditions, however, can-
not reflect what happens in daily life, and to this aim,
24-hour BP and HR recordings performed in ambulant
subjects have to be considered. Analysis ofthese record-
ings may provide a description of the day-night modu-
lation of fast (ie, 0.025 Hz) BP and HR spectral
‘components. This can be obtained by time-varying spec-
tral analysis techniques, such as the sequential spectral
approach or the Wigner-Ville technique,2*?" all of
which track the time-varying features of BP and HR over
the recording period. Use of these techniques allows the
BP and HR spectral responses to behavioral and envi-
ronmental factors to be identified (Fig 4). Through the
analysis of 24-hour ambulatory BP and HR recordings,
information on slower components of BP and HR
variability can also be obtained. This can be achieved by
using spectral techniques that provide a single speetrum
from the entire 24-hour recording, thereby estimating
spectral components over a broad range of frequencies
(broadband spectral analysis, Fig 5).%+° This allows
one to collect information on ultrasiow HR and BP
changes and on their potential relevance to cardiovas-
cular control mechanisms. The broadband approach, for
example, has led to the important finding that 24-hour
BP and HR spectra are characterized by a l/f
trend"; je, the amplitudes of BP and HR fluctu
tions increase progressively with the reduction in the
frequency of such fluctuations. This spectral character-
istic indicates that overall 24-hour BP and HR variabil-
ities depend more on very low than on higher frequency
components. The I/f trend of BP and HR spectra has
also been shown to undergo marked changes indifferent
pathophysiological conditions:
Interpretation of Spectral Data
Spectral analysis techniques used to quantify BP and
HI variability usually focus on the variability compo-
nents with frequencies ranging between 0.025 and 0.50
Hz, based on the evidence that in these frequency
regions, BP and HR spectra are at least in part modu-
lated by neural autonomic influences“ Despite the
large number of studies available on this issue, however,
the interpretation of the BP and HR spectra in this
frequency region is still a matter of some debate
Interpretation of HR Spectra
‘Vagal cardiac control operates like a low-pass filter
with a relatively high cutoff frequency, effectively mod-
ulating HR up to 1.0 Hz, while sympathetic cardiac
control operates as a low-pass filter with a much lower
cutoff frequency, capable of significantly modulating HR
only at frequencies below 0.15 Hz. The results of a
‘number of studies support this view. In dogs, broadband
electrical stimulations of the vagus are followed by HR
changes with minimal dampening up to at least 0.7 Hz,
whereas broadband electrical stimulation of the right
Parati et al Cardiovascular Control and Spectral Analysis 1279
stellate ganglion is followed by TIR changes with a delay
Of approximately 2 seconds and a dampening that leads
to @ minimal response above 0.15 Hz" Second, in
dogs and humans, parasympathetic blockade by atropine
‘eliminates most HR fluctuations above 0.15 Hz, while
Teaving those below 0.15 Hz partly unaffected."
10!
wo
ot
wo
Brot
So
E10
10
1
10
0
ws rt tot 107
He
Fic 5. Plot shows broadband spectrum of systolic pressure
bbtained from the analysis of a 24-hour ambulatory intra-arterial
blood pressure recording performed in a normotensive volun
tect, Spectral components with fraquencies ranging from 1 to
‘ppronimately 0.000023 Hz (e, with periods ranging from 1
‘Second fo 12 hours) are considered. The continuous line refers
to the actual spectra; the discontinuous line is the 1/1 tine
modeling the spectrum in the frequency region where the 1/F
‘model is suitably applicable.
inours)
Fred. Plots show soquentil power spectrum den-
sities (PSD) of low-frequency (0.026 to 0.07 Hz},
mmid-frequency (0.07 to 0.14 Hz), and high
ftequency (0.14 to 0.85 Hi) systolic blood pressure
(SBP) oscillations computed over consecutive seq-
‘ments of 256 beats throughout a 24-hour period in
‘2 representative subject. SBP mean values and
Standard deviations for each half hour ofthe recor
ing are also shown. Data are derived trom a 24-hour
intraartenal ambulatory blood pressure recording
‘of a representative subject. Dotted lines inthe right
panel refer to sagments in which PSD could not be
Estimated because of nonstationartios in the re
‘Corded signal. (From Paral eta" by permission)
Third, cardiac sympathetic blockade with propranolol
reduces HR fluctuations below 0.15 Hz, while leaving
those above 0.15 Hz largely unalfected.=**3” Thus, HR
changes at frequencies above 0.15 Hz seem to be
primarily caused by modulation of cardiae vagal efferent
activity. Also, since respiration usually occurs at frequen-
ties greater than 9 breaths per minute (0.15 Hz), respi
ratory fluctuations in HR are likely to be mediated
primarily by parasympathetic efferent pathways. These
‘observations explain the use of respiratory sinus arrhyth-
mia as a measure of cardiac vagal modulation.® 44”
However, they also explain why respiratory sinus ar-
rhythmia’ may not accurately reflect only vagal HR
‘modulation, since sympathetic modulation of respiratory-
induced HR changes occurs when the respiratory aetivity
is below 0.15 Hz. Finally, even at frequencies above 0.13
Hz, not all HR modulation is parasympathetically me-
diated, A small respiratory sinus arrhythmia postulated
to be caused by mechanical modulation of sinus rate by
stretch persists after combined pharmacological sympa-
thetic and parasympathetic blockade and alter cardiae
transplantation2=!" One can thus conclude that HR
power in the HF band, above 0.
but incomplete measure of vagal cardiac control
‘The specificity of LF and MF HR powers for a single
control mechanism is even lower because (1) in animals,
HI fluctuations at frequencies below 0.15 Hz are af
Vy ‘and sym-
pathetic cardiac nerves™=*; (2) in humans, HR powers
between 00.03 and 0.15 Hz are reduced by either para
sympathetic or sympathetic pharmacological block-
‘ide229"; and (3) HR fluctuations in this region have been
associated with a wide variety of stimuli, including
1280 Hypertension Vol 25, No 6 June 1995
thermoregulation, periodic breathing, and hemody-
namie instability.%5* Thus, HR spectra in the MF or LF
regions are not invariably a specific sympathetic marker,
it has been suggested,%= but may also depend on
‘vagal influences and other mechanisms. The reliability of
these spectral indexes in reflecting cardiac sympathetic
modulation can be enhanced, however, in a number of
behavioral or experimental conditions in which the
sympathetic system can be selectively activated.®+*
Interpretation of BP Spectra
‘The observation that HF BP power is not substantially
modified in patients with denervated donor hearts! 343
has led to the suggestion that this power is mainly caused
by the mechanical effects of respiration on the pressure
gradients, size, and functions of the heart and large
thoracic vessels25 There are, however, conflicting
findings on this issue. Actually, it has also been sug-
ested that vagally mediated changes in HR and cardiac
output play a role in determining HF BP powers
However, the influence of vagal modulation on HF BP
powers may be different in different species because in
‘conscious cats, sinoaortic denervation, ie, an interven-
tion that markedly impairs cardiac vagal drive, markedly
reduces HF HR powers with only a minor and nonsig-
nificant reduction in HF BP powers.”
‘Autonomic modulation of HR is an even less impor-
tant determinant of BP powers in the LF and MF
regions because cardiac autonomic blockade by the
combined administration of atropine and propranolol
climinates only a fraction of BP variability at frequencies
lower than 0.15 Hz2? It thus seems likely that LF and
ME BP powers are predominantly caused by fluctuations
in vasomotor tone and systemic vascular resistance. At
frequencies between 0.25 and 0.07 Hz, the factors
wolved in this vascular modulation have been regarded
as being the renin-angiotensin system, endothelial fac-
tors, local influences related to thermoregulation, and
others.2"5%*! However, their precise role remains largely
speculative. In contrasi, evidence has been collected that
in the frequency region between 0.07 and 0.15 Hz (or
between 0.05 and 0.15 Hz according to other authors),
BP powers increase with laboratory stimuli that increase
sympathetic cardiovascular influences (eg, head-up tlt-
ing, mental stress) and decrease with conditions that
decrease sympathetic cardiovascular influences (eg,
sleep and a-adrenergic blockade).*”-» Thus, the hy-
pothesis has been advanced that the BP spectral powers
between 0.07 (or 0,05) and 0.15 Hz (defined as LF or MF
by different investigators) represent a marker of sympa-
thetic vasomotor tone. As mentioned above, the same
type of evidence (increase and decrease in power during
increase and decrease in sympathetic drive) has been
used to conclude that HR powers in the same frequency
region represent _a marker of sympathetic cardiac
drive. However, as is the case with HR, LF (or MF)
BP power may not invariably be a consistent marker of
sympathetic vasomotor regulation.
BP and HR Spectral Powers as Indexes of
Autonomic Cardiovascular Modulation
Markers capable of dynamically assessing sympathetic
vasomotor and cardiac drive in daily life conditions
would be important diagnostic tools" However, the
reliability of BP (or HR) powers around 0.1 Hz as
specific sympathetic markers has revently been ques-
tioned by several investigators. Their data come not only
from animal experiments, which have the problem of a
safe extrapolation t0 humans, but also from healthy
subjects and patients with cardiovascular disease. For
example, Cohen et al® reported that in healthy volun-
teers a reflex increase in sympathetic nerve trafic (mea-
sured directly by microneurography) and in vascular
resistance (measured by forearm venous oechision peth=
ysmography) induced by lower body negative pressure
‘was not accompanied by a similar consistent increase in
0.1-Hz HR power. Saul et a found that in normoten-
sive humans the reflex increase in sympathetic nerve
trafic (microncurography) induced by intravenous infu-
sion of nitroprusside was associated with an increased
0.1-Hz HR power but that no reduction in the 0.1-Hz
HR power occurred during the reduction in sympathetic
nerve trafic reflexly induced by intravenous infusion of
phenylephrine. Kingwell et al showed that although i
some clinical conditions (early heart transplantation and
pure autonomic failure) cardiac norepinephrine. spill-
over and 0.1-Hz HR power were concordant reduced,
in other clinical conditions (late heart transplantation,
‘aged individuals, and congestive heart failure) they
showed discordant changes. Kienzle etal observed that
in heart failure patients there was an inverse correlation
between different measures of HR variability, including
0.1- and 0.3-Hz powers, and indexes of sympathoexcita-
tion such as muscle sympathetic nerve activity and
plasma norepinephrine—ie, the higher the sympathoex-
citation, the lower the powers of 0.05 to 0-15~ and 0.2 0
O.5-Hiz HR spectral components and the HR standard
deviation. Daffonchio et al observed that in conscious
rats destruction of the peripheral sympathetic nerves by
‘-hydroxydopamine reduced the 0.2 10 0.8-Hz BP pow-
ers (ie, the powers corresponding to the powers around
0.1 Hz in humans) by 65% in normotensive rats and by
only 20% in hypertensive rats, the remaining power
boeing unalfected by the elimination of residual sympa-
thetic activity and adrenal gland influences via additional
awvacrenergic blockade. Finally, Adamopoulos et al®?
also showed that in patients with congestive heart fail-
ure, spectral indexes of autonomic activity correlate
poorly with other measures of autonomic function
‘The important conclusion that can be drawn from
these observations is that the level of sympathetic car-
iovascular modulation cannot always be specifically
reflected by the power of HR and BP spectral compo-
nents around 0.1" Hz.
‘A further important issue to be considered is the
reproducibility of these spectral indexes. Although some
studies have teported that, in standardized conditions,
O.1- and 03-Hz powers of BP and HR have a good
reproducibility other studies have emphasized the
Possible occurrence of a high random variability in BP
‘and FIR spectral powers even when derived from stan-
dardized recordings.”:” Reproducibility of BP and HR
spectral powers in the 0.025 to 05-Hez region is an even
‘more complex problem when these spectral components
are quantified, in individual subjects, from the analysis of
short-lasting segments derived from 24-hour ambulatory
BP and HR recordings because of the influence of
varying behavioral conditions 278
Other more general problems related to the use of
spectral powers as tools for selective quantification of
Parati et al Cardiovascular Control and Spectral Analysis 1281
autonomic cardiae or vascular influences are worth
mentioning. First, neural modulation of both HR and
BP is influenced by a large number of input signals and
diversified interaction of central command and reflexes
at various brain levels. Thus, it may be that an approach
Which assumes that these complex mechanisms can be
described by considering only BP and HR spectral
powers within the narrow frequency regions around 0.1
and 0.3 Hz is too simplistic. Its more likely that a much
wider frequency region, containing rhythmic and non-
shythmic fluctuations, is under the modulation of these
neural mechanisms, a hypothesis that has some support
in the literature, When broadband spectral analysis has
been used for the assessment of BP and HR variability in
conscious cats and dogs, arterial baroreflex regulation of
BP and HR fluctuations has been found to occur at all
frequencies, from the very low to the very high."
Second, the current interpretation of spectral data
relies on the assumption that the responses of the system
‘under evaluation are approximately linear. Yet, neural
regulation of the cardiovascular system is characterized
by at least two orders of nonlinearity. There are system
nonlinearities, present regardless of the operating point,
such as the nonadditive nature of the interactions of
cardiac sympathetic and parasympathetic responses,”
the cardiac phase-dependent response of the slope of
phase 4 depolarization to vagal stimuli’* and the possi
ble nonlinear gating of vagal and sympathetic neural
outflow by respiration.” In addition, there are nonli
cartes that may originate in specific behavioral and
experimental conditions, driving the cardiovascular sys-
tem control mechanisms to operate out of their linear
range. Virtually every physiological control system has
steady-state responses that are sigmoidal and include a
threshold, saturation point, and in between, a linear
‘operating regime” (Fig 6A and 6B). A typical example
of this is represented by the arterial baroreflex control of
HR, which has a sigmoidal stimulus (BP)-response (RR
interval) curve. In this instance, both the steady-state
and dynamic responses of the system are a function of
the BP level. The dynamic response can be thought of as
continuously moving up and down the sigmoid curve
that describes the steady-state baroreflex gain, with
‘maximal gain usually equal to the instantaneous slope of |
the sigmoid curve (Fig 6C and 6D). In addition, the
system gain at any one mean operating point might
depend on other factors, such as the frequeney with
which the input varies (eg, low-pass filter responses to
sympathetic modulation) or the rate of change of the
input (eg, wiss differentiator properties of the
arterial baroreceptors to phasic inputs).” Fig 6C shows
clearly that an increase in the mean operating point of
decrease,
‘or no change in the dynami depend
ing on the initial operating point, a parameter that
‘annot be determined by means of a simple frequency
domain analysis, This implies that changes in the activity
Of cardiovascular control mechanisms (which, as already
mentioned, are often intrinsically nonlinear) may not be
lincarly related to changes in BP or HR variability. Thus,
‘a measure of BP or HR fluctuations may fail to qu
alterations of autonomic cardiovascular influent
several instances. OF course, this may be a problem of al
measures of autonomic tone in relation to its modulating
Static (Steady State) Gain
aa} rg can,
eS =
BF ian BF
Dynamic Gain
je D
RR Gain, eee
(rnceci} maul mmHg)
ome a
Fic 6. Schematic drawing shows diferent features of the sen-
sitivity (gain) of baroretex heat rate control. A, Sigmoid curve
‘escrbing the relationship between changes inthe Input (bI00d
pressure, BP) and reflex changes in the output (RR interva). AS
BP increases, RR interval also increases, approximating a sig-
‘moidal reationship wth threshold and saturation values at ether
tend ofthe curve, Me gain of the heat rate baroreflex is defined
fa the slope at any given point on the response curve. Admin=
istration of vasaetve agents (nitroprusside [NP] or phenyloph-
fine [PE induces changes in moan arterial pressure, moving the
rormal baroreflex operating poi (baseline) into. a. diferent
‘perating range. This potentially may lead to diferent gains. B,
Plot of baroreflex steady-state gain as a function of BP. As the
‘baroreflex stimulus-response curve s sigmoidal, maxim gains
‘observed inthe linear portion of the curve, occurring a interme
bate BP values. At more extreme SP values, steady-state gains
Cinished. C, Dynami (or “bea-to-beat) baroreflex gain as
meaured by the autoregressive moving average (ARMIA) the
Spectral and the sequence techniques at the mean operating
pint in A may be higher or lower than the steady-state gain,
Bepending on the characteristics of the BP signal. , in partic
Ur, the dynamic gain will probably depend on the trequency
Content of the Input signal because of either inherent fering
Characteristics of the Barorellex response (e, low-pass, high-
pase, band-pass) or dependence on a signal derived from the
Input, such as the dervative or rato of change of the input signa
Inthis case, maximal gain is found to occur around 0.15 Hz, wth
‘ocreased gain at both ends ofthe frequency range, suggesting
band-pass characterstics.
influences and to its effect on receptor, cardiac, and
vascular responses.
As_a somewhat separate issue, frequency domain
techniques are particularly suitable for the measurement
Of dyntamic responses. Thus they may not be appropriate
for the assessment of mean operating conditions in the
system under evaluation. This is particularly the ease in
the evaluation of the sympathetic or parasympathetic
‘modulation of HR of BP, in which spectral analysis is
unlikely to provide a measure of mean neural activity,
This point is graphically demonstrated by the response
of respiratory sinus arrhythmia to an elevation of mean
arterial pressure induced by an infusion of phenyleph-
rine (Fig 7). In this case, mean vagal activity almost
certainly increases (HR decreases by approximately 18
June 1995
ee
Time (in) Time (in)
Fia 7. Plots show time series of respiratory volume (top),
heart rate (midland mean blood pressure (bottom) in one
Subject. Data wore obtained in contr conditions (let) and
{during intravenous phenylephrine infusion (ight), which do-
termined an increase in blood pressure and a reflex bradycar-
dia. Note that at the time of maximal reflex cardiac vagal
stimulation under phenylephrine infusion, respiratory sinus
arrhythmia disappeared.
beats per minute), but respiratory. sinus arrhythmia
isappears, probably secondary to the saturation of
either the Vagal responses or the response of the heart to
vagal activity (LPS, GP, unpublished observations,
1994).
Finally, two further methodological issues deserve to
iscussed in this context. First, proper interpretation
is highly dependent on the presence of
signal stationarity." This issue is more than a theoretical
requirement for the use of spectral analysis any time the
attention is focused on specific spectral peaks because
the dynamic characteristics of the system are likely 0 be
diferent during changes in the mean operating point
Second, interpretation of the spectra also depends on
the occurrence of an appropriate degree of spontancous
fluctuations of the parameters that influence the signal
under evaluation so that the risk of having no input data
in the frequency range of interest is avoided.="08 A
proper degree of variability in the input data can be
obtained by recording the signal under changing external
stimulations. As an example, this ean be done by using
paced breathing over a wie frequency range as a means
to elicit variations in the cardiovascular signals and in
the engaged control mechanisms.
Closing the Gaps
‘The most common attempt for improving the assess-
ment of autonomic cardiovascular modulation by the
spectral analysis approach is to couple the information
obtained from the recorded biological signal with the
information derived from physiological and mathemati-
cal models. This may help the interpretation of the
results, provided that the model (1) is used when its
assumptions fit with the biological data and (2) is
validated at least in part by experimental data indepen-
dently obtained. An example is a model based on the
assumption that sympathetic and vagal cardiac influ-
fences are normally altered in opposite directions and
that thus one can improve on the limited sensitivity of
0.1-Hz (LF or ME, according to different authors’ defi-
nitions) and 0.3-Hz (HF) powers as respective markers
of sympathetic and vagal cardiac drive by using their
ratio as an index of sympathovagal balance. Such a
model may provide useful information in a number of
instances. However, there may be conlitions (eg, eX-
ecise, diving) in which these two spectral components
undergo not discordant but concordant changes of sim-
ilar or different magnitude. In the latter ease, the
resulting changes in the LF-HF ratio may be misinter-
preted as indicating opposite changes in sympathetic and
vagal drive
Other more complex examples are the modeling ap-
proaches that consider the relationship between fluctu-
tions of two oF more cardiovascular signals physiolog
cally related to each other. To date, these multivariate
models have allowed evaluation of the baroreceptor-HR
reflex using both time domain and frequency domain
approaches. A time domain method described in the
1980s" is based on computer identification of se-
quences of three or more consecutive beats character-
ized either by a progressive increase in systolic BP
followed by a linearly related lengthening in. pulse
interval or by a progressive reduction in systolic BP
followed by a linearly related shortening in pulse inter-
val. The slope of the regression line between systolic BP
and pulse interval changes is taken as an index of
baroreflex sensitivity. A frequency domain method also
used to assess baroreflex sensitivity is based on the
computation of the squared ratio between the spectral
powers of RR interval and systolic BP® or of the
‘modulus ofthe cross-spectrum between systolic BP and
RR interval in the frequency regions (0.07 to 0.35 Hz)
where these two signals show a significant coherence **
‘The validity of either approach has been independently
verified by the striking changes in the outputs of these
models produced by sinoaortic denervation in ani-
mals, which allows their use as a reliable index of
baroreflex sensitivity in daily lie.
Other multivariate models are (1) those addressing
the relationships between BP and HR in a closed-loop
fashion, by means of either autoregressive moving aver-
age techniques (ARMA models)" or Fourier-based
transfer function techniques, and (2) those quantifying
the relations between respiration and either BP or HR.
fluctuations using the same techniques." Inthe former
instance, ARMA. models have been used to study not
only the reflex effects of BP alterations on HR changes
(reflex feedback) but abo the direct mechanical effects
of alterations in HR on BP changes (mechanical feed-
forward). On the other hand, with either technique, the
evaluation of the relation between respiratory activity
and BP or HR changes can be used to provide a
quantification of the gain and phase relationship be-
tween respiration and its cardiovascular effects as a
function of the frequency of these changes. This ap-
proach may be further improved if the analysis is not
limited to spontaneous respiratory activity (which may
have a limited frequency content) but makes use of
paced breathing pattern to obtain a broadband or “whit-
ened” input respiratory signal that contains all physio-
logically relevant frequencies simultaneously (see
above)”
BP and HR Variability in
Essential Hypertension
Using short-lasting BP and HR recordings obtained in
the laboratory environment, Guzzetti et al" reported
Parati cs al Cardiovascular Control and Spectral Analysis 1283)
that, compared with normotensive subjects, patients with
essential hypertension are characterized by a greater LF
power (defined as the power around 0.1 Hz) and a
smaller HF power of RR interval during supine rest.
‘They also reported that these powers showed a smaller
increase and decrease, respectively, during passive tilt
ing. These observations were interpreted as indicating
that cardiac sympathetic tone is incre
vagal tone and modulation are decreased in esser
hypertension, a conclusion in line with the previous
studies in which autonomic cardiac modulation was
investigated by different techniques." They also con-
cluded, however, that sympathetic cardiac modulation
‘may be impaired in hypertension, wl
agreement with previous reports showing unchanged
and even enhanced HR responses to exercise, stress, and
‘autonomic cardiae drive.
Comparison data are alo available on BP and HR,
variability of normotensive and essential hypertensive
subjects throughout the 24 hours. In a study that made
use of 24-hour intra-arterial ambulatory BP ceconding,
sively from normotensive subjects to pat
derline, mild, and more severe essential hyper.
‘The HR standard deviation was similar in normotensive
subjects and in borderline and mildly hypertensive pa-
tients and decreased in severely hypertensive patients.?
Further results were obtained in additional studies in
which the 24-hour intra-arterial BP and HR signals of
normotensive and hypertensive subjects were divided
into contiguous segments of 5 to 6 minutes, and power
spectral analysis was performed on all segments charac
y ary signal.22” In all subjects, spectral
powers displayed a large segment-to-segment variabil-
ity over the entire frequency region considered, pre-
sumably because of the effect of the changing bel
ioral pattern, Spectral powers, however, also showed
ematic fluctuations, which consisted of (1) a pro-
nounced nocturnal reduction of the systolic and di
stolic BP powers around 0.1 Hz and (2) a more slight
nocturnal increase in the 0.3-Hz (HE) power of pulse
interval. With the exception of a smaller
increase in the HE power of pulse interval, average
powers and power changes were similar in the normo-
tensive and mildly hypertensive subgroups.2°2?
Finally, the time domain and frequency domain tech-
‘niques for computer evaluation of the arterial baroreflex
described above®?*5* have shown that the sensitivity of
the baroreceptor-HR reflex is much lower in essential
hypertensive than in normotensive subjects for each
hhour of the 24 hours, thereby confirming previous con-
clusions obtained by studying the baroreflex with labo-
ratory techniques." Dynamic analysis of the baroreflex,
however, has also shown that although in normotensive
subjects baroreflex sensitivity shows a marked nocturnal
increase, this feature is much less evident in hypertensive
data obtained by quantification of BP and HR
fluctuations in hypertensive pationts emphasize that,
although interpretation of the results may not always
be easy (mainly because of the composite nature of
spectral powers), time domain and frequency domain
analysis of HR and BP variability can provide inter.
esting new insights into the daily life alterations of
autonomic cardiovascular modulation in hyperten-
sion. A striking finding appears to be a daily life
impairment of the baroreceptor-HR reflex. There are
also an increase in BP variability and to a lesser extent
a reduction in HR variability. These alterations are
more evident when overall measures of BP and HR
variability rather than specific components of these
phenomena are considered.
Conclusions
Available data unequivocally indicate that analysis of
BP and HI variability by the spectral approach, as well
as by time domain techniques, may provide interesting
information and represent a useful tool for the study of
the mechanisms involved in cardiovascular regulation in
both normal and diseased conditions. The potential
importance of these techniques is in particular related to
the possibility they offer for information to be obtained
on cardiovascular regulation in real life conditions, i, in
conditions free from artificial laboratory stimulations.
However, interpretation of BP and HR spectra is some-
times controversial, particularly when signals recorded
‘outside of a standardized laboratory environment are
considered, and there is evidence that specific spectral
components may he related to different mec
different conditions. In particular, although sympathetic
vascular and cardiae modulation appears to be reflected
by BP and HR powers around 0.1 Hz, the specifi
sensitivity, and reprod
dewes of mean sympathetic activity in different condi
tions are not always optimal. Progress in the field is now
oollered by multivariate models that allow interactions
between BP, HR, and other biological signals to be
cevaluated in the time or frequency domain, Application
Of some of these models to the analysis of long-lasting
BP and HR recordings obtained in ambulant subjects
will also allow the problems arising from the use of
laboratory data to predict what happens in daily life 10
be overcome.
Appendix A
Removal of Artifacts
Recordings of BP, eleetrocardiographic, a "
signals may inchude artifacts, such as dampening of the BP
Signal, distortion of the pulse waveform by movements, pre
{ure beats, ete. The likelihood of these urtifets being found in
the recorded signals is obviously higher when Tongesting
recordings are being considered, particulary if these record
ings are obtained in smbulant subjects
‘ high frequency of arifets also must be expected when
long-lasting recordings obtained by a Finapres measuring de-
vice (Finapres 2300, Ohmeda) oF by’ iis portable version
(Portapres, TNO) are considered because the site of BP
measurement, atthe finger level, is associated with «high rate
fof movement artifacts” and hecause the continuous BP
recording is periodically interrupted by automatic calibration
signals
These artifacts must be removed to obtain reliable spectral
‘estimation, and signal editing is particulary crucial to avoid
crtors in the quantification of faster HI and BP spectral
components
‘Occasional ectopic beats can be removed by
procedures: (1) Interpolated. cetopie beats
removed, and the RRC interval corresponding to the missing
beat will then be the sum of the intervaly preceding. and
following the ectopic beat; (2) if a delay follows the ectopic
beat, the RRC interval considered for analysis might be the
1284 Hypertension Vol 25, No 6 June 1995
mean of the intervals preceding and following the removed
‘ectopic beat. Such a procedure is particularly suitable for
ectopic beats followed by a compensatory delay. Obviously,
recordings without arrhythmias should generally be preferred.
Incase of long-lasting recordings (eg, 24-hour Holter tracings),
fan acceptable riterion might be to consider for spectral
analysis only subperiods during which the frequeney of ectopic
beats is less than 1% of total beats,
“The editing task can be efficiently performed through com-
puter identification of aberrant waveforms. This is commonly
obtained (1) by setting threshold values for specific fiducial
poinis on the recorded waveform (eg, in the case of BP
recordings, the maximal and minimal values for systolic and
diastolic BPs, the maximal and minimal time lengths ofa given
‘waveform, rte of change of BP within the waveform, ete) and
(@) by matching each recorded waveform with a template.
‘Once detected, artifacts can be either automatically deleted
by the computer or visualized on a screen and interactively
doleted by the operator.
Appendix B
Essential Glossary
Autoregressive (AR) Modeling
‘Technique for the mathematical modeling of signals, This
approach is based on the assumption that the value ofa signal
depends only on the previous values of the same signal plus
“noise.” Once the AR model of a signal i estimated, the
spectrum ofthe input signal canbe computed from a manip-
Ulation of the mathematical mode.
Autoregressive Moving Average (ARMA) Modeling
‘Technique for the mathematical modeling of signals. I i
based on the assumption that the value of the output signal
depends on either the previous values of the same signal
{autoregressive component) and on the present and previous
values ofa diferent input signal (moving average component),
withthe addition of "noise" factor.
Broadband Spectral Analysis
Speetal analysis proving a spectral estimation over a wide
range of frequencies. By this approach, a single spectrum is
obtained from a relatively long-lasting input data record
Fourier Transform
Decomposition of a given signal into a series of sine and
cosine waves having frequencies that are multiples of the
fundamental frequency (the reciprocal of the time length of the
input data record). The spectral power ofthe input signal ean
bbe derived from the magnitude of these sine and cosine waves.
Fast Fourier Transform
Algorithm fo the fast estimation of the Fourier transform. It
roquires that the number of samples derived from the input
signal be powers of 2
‘Set Point
‘The specific value of the controlled variable that should be
‘maintained by a given control mechanism (eg, the arterial
barotefey).
Time-Varying Spectral Analysis
A set of analysis procedures that describes how the spectral
‘characteristics of the input signal change as a function of time.
Transfer Function
Mathematical relationship between the input and output of a
system as 2 function of the frequency.
References
1. Guyton AC. Textbook of Media! Physiology Pildelpia, Pa: WB
LL Parati G, Pomidosi G,
Bertinit! 0, Grasi G, Di Rienzo M, Pedoti A, Zanchets A
Blood pressire and heart rate varaiies im normotensive and
Inypertensive human being. Cie es. 1983,5396-108,
Mineia G, Zancheti A. Blood pressure variability. In; Zanehet
A.Tarazi R, eds Handbook of Hyperonsion. Amsterdam, Neth
sands Eker Science Publishing Co, Ine: 19867 125-152
4. Akseod 8, Gordon D, Ute! FA, Shannon DC, Barger AC, Coben
RU. Power spectrum snalss of ear ate Mocwations: a quan
tive probe of beat-to-beat cardiovascular control. Scene,
rosi2h2900%2
5. Appel ML, Berger RD, Saul JP, Smith IM, Cohen RJ. Beat 9
tet variability cardiovasculae variables: oie or matic? J Am
Coll Cail. 19894 141139-1198,
Malian A, Pagani M, Lombardi F, Cert $. Cardiovascular
ural rsition explored in the frequency domain. Civulation
Toor:se2492
7. Part G, Muti E, Omboni S, ManciaG. How to deal wit blood
‘ressre variability. In: Brunner H, Washer B, eds. Ambulatory
‘Blood Pressre Recordin, New York, NY: Raver ress Publishers;
oor,
A. Marcia G, Di Rienzo M, Parti G. Ambulatory blood pressure
‘monitoring use in Iypertesion research and einical practice
Hyertenson, 1993.21 510-52,
9. Litér WA’ West MJ, Hovour AJ, Sleight P. The variability of
ston presse. Am Heat J 197895180185.
10, Cowley AW, Liard LE, Guyton AC. Role of the baroreceptor
feller in dally contol of arterial blood pressuee and other
Yaribles in dogs. Cire Res 197332:564576
11, Jenkins GM, Walls DG. Special Anais and ly Applications
Oakland, Calf: Holden Day: 1968
12 Kay SM, Marple SL. Spectrum analsis: a modem perspective.
Proc IEEE. 1981:8:1380 118.
13, DiRlenzo M, ManciaG, Parati G, Pedoti A, Zancheti A, ed
Blood Presute and Heart Rate Variability Amsterdam, Net
cerns: 10S Press 192
1M, Hales Stradey: Conmaining Hacmasaticks London, UK:
Fanny, Manby and Woodsard: 17332.
15. von Haller A Elemente Psiolgiea, Lausanne, Stern: 1760;
Tit, ut vi, 330"
16. Koepcten HP. History f stues and concepts of blod pressure
waves. I: Miyakava K, Koepehon HP, PolosaC, eds. Mechanisms
9f Blood Pressure Waves. ‘Tokyo, Japan/Berin, FRG: Japan
Science Society PressSpringr-Veriag: 1988:3-2,
17. Mayer 8. Studien zur pisioiogic des herzens und der blugetase,
‘5: Abhandlung’ Uber spontane blutdeockschvankungen, Sher
“Akad Wise Wien, 189674281-307,
18 Penne J. Miner waves: history and methodology. Auomedin
17821364.
1, Sayers BMCA. Analysis of heart ate vasabilty rgonomis. 173;
Wwrrs
20, Hyndman BW, Kitny RI, Sayers BM. Spontaneous rhythms in
plysologcal contol systems Nature. 1971238394
21, Akeld 8, Gordon D, Madwed JB, Snidan NC, Shannon DC,
CColea RJ. Hemodynamic regulation: investigation by spectral
analysis. Am J Pil 1985:289:H 857-18,
22, Sou IP, Berger RD, Albrecht P Stein SP, Chen MH, Cohen RU
Transfer fanetion ana of the cielaion- unique insights into
cardiovascular relation. Am J Psi. 1991-2614 1281-H125,
23, Pagani M, Lombardi F, Guzet 8, RimoldiO, Furlan R, Pix
zine P, Sandrone G, Malfato G, Delo, Piealuga E,
‘Tutiel M, Baset'G, Ceruti 8, Mliant A. Power of spectral
nals of heart rate and arterial pressure variables sa marker
‘of smpatho-ragal interaction in man and conscious dog. Cire Re
1986;38178.198.
24, Berger RD, Saul JP, Coben RU. Transfer funtion analysis of
autonomic regulation, I eanine ati ate response rd Psa
Ioso.asec1ta2 152
25. Di Rienay M, ParatiG, Castigon! P, Omboni S, Feri AU.
Ramirez AJ, Pedot A, Manca G. Role of sinoaoi afferents
‘modulating BP and pulse Interval spectral analjis in unanes.
thetized cats. Am J Physio. 1991261 1811-1818
25, Dj Rienzo M, Cation P, Manca G, Para G, Pedott A. 24
Hour sequential spectral anal of arterial biol pressure and
Pube interval i foe-moving subjecs. ZEEE Trans Biomed Eng.
Foss 1046-1075,
6
Paratiet al Cardiovascular Control and Spectral Analysis 1285
Parati G, Cason P, Di Rienzy Mt, Omni S, Podout A,
“Mansa G, Sequential spectral analysis of +hour bod pressure
and pulse intra in amas Hyperenson. 1990:16:1 421
Bergland GD. guide our ofthe fst Fourier transform, FEE
Speen. July 6, 1HD1-52
Boe GEP, Jenkins GM. Tine See Anabsie Foecasig and
Cont. San Franco, Calif Holden-Day, 1970.
Kay SM. Modern speetal estimation: theory and application.
Englewood Clifs, NI: Preaiee Hall 1988
Kashyap RL. Inconsistency of the AIC rule for estimating the
order of autoregressive models IEEE Trans Ausomat Con
12s 96.97
2, Blackman RB, Tukey JW. The Measurement of Power Specia From
the Pot of View of Communication Engineering, New York, NY:
Dover, 1959,
Furlan R, Guzzeti S, Crivellro W, Dass S, Tiel M, Basel G
‘Gera S; Lombard F, Pagani M, Malian A. Continuous 24-hour
sssessment of the neural regulation of stem eral pressure
fn RR varies in ambulant subjects. Ceulaion, 190:
SHS?
Bianchi AM, Mainard L, Petre E Slnorini MG, Minar M,
‘Gert §,Time-variant power spestcum ana forthe detection
of transcat episode of HRV signal MEEE Trans Biome! Eng
Io9SsHh 136-14,
Yana K, Siul JP, Berger RD, Perrott MH, Coben RJ. A time
domain approach for the fitGaton nals of hear at ate
{o instantaneous lng volume, IEEE Trans Blom Bg. 19340:
Ta
36. Cohen L. Timefrequency dicibutions: « review, Proc IKE.
1989:77 941 981
‘Venturi M, Confort F, Macerata A, Varanini M, Emin M.
Marchest C. Analysis of vanibilig: a sjsem fr comparing
‘Slaw, parameti, apes and Wigner Vile power spocttal
stmt Ine Pr’ Comp be Candy Los. Alamitos. Cali
IEEF Computer Society Pres 199124728
Kolryaahi Mt, Muska. 1 factuations of heartbeat period IEEE
Trans Biomed Eg. 198220:456457
Saul JP Aboot P, Berger RD, Cohen RJ. Analysis of ng erm
heart rte variability: methods, 1 sealing and implications. tn
Proc Camp in Cartolg Les Alamitos, Calf: IEEE Computer
Society Pree, 19864155021
Person P, Eke 11, Kholer WW, Kichcio HR. Ientication
‘f major dow Hood presse exellations i conscious dogs: Am
Pro. 1990289 HOS AISS,
Goldberg AL, Rigney DR, West BJ, Chaos and fractals in human
pony Se ir 1900:9:450,
w. Di Rienzo M, Castghoni P, Parati G. Role of the arterial
Ibarorfes in poking the Tif shape of systolic loot! presse
‘pt. In: Proc Comp Caro Los Ala,
Computer Society Press 199225328.
Di Rieazo M, Castigiont P, Frattoln A, Mancia G,
Pedotti A Elects of 4h mulation of baroreflex sn on
Wood! pressure variability. In: Prac Comp tn Cardia Las
‘Alanis, Calf, IEEE Computer Society Press 193:551 354
Saul JP, Rea RF, Exhberg DL. Berger RD, Coben 8 Heat rte
fn muscle sympathetic nerve varatiy daring rellex changes of
ftonomic aot. J Pe. 1980-28817 13. 72)
Lombardi F, Sandrane G, Perpaner 8, Sala M, Garimoldi M,
(Cerutt, Bisel G, Pagani M, Malian! A Heart sate variability
‘am index of sympath-agalinteracon ater acue myocardial
infarction in J Carl 187 0:1239-125,
‘Saul JP: Bea o-beat variations of hear rate rest modulation of
‘cardiac autonomic cutflow, News Pao! Sei. 1995327
Fouad FM, Tarsst RC, Ferrario CM. Fighaly S, Alcandei C
Accssment of parasympathetic control ot heatt rae by a Hon:
sho. ie) Physi. 184 2468S.
una sinus arith as an index of vagal eariac
futon J Appl Phys. 198338 901-96,
Katona PG, Sth F. Respiraiory sinus arhythmis, noninvasive
measure of parasympathetic cardi citeol J App Pil.
1075;3 80.05
Saul JP, Merger RD, Chen MH, Cohen RJ. Transfer function
‘mals of autonomic ogultion, UI eespitatory sins arta
dm Piso. 1980286418341)
‘Bernal LF, Keller M, Sanders M, Reddy PS, Meno F, Pinsky
[MIC Respiratory siousarshytmia in the denervated human hear
J Appl Physi. S677 1,
Deliver RW, Karomaker IM, Stackee J. Hemodynamic Hutu
loos and baroreflex sensiviy inhuman: a beat-to-beat model,
fim J Physio. 198725920680 168,
153, Petes J, Fraser C, Sturt RS, Baumgartner W, Robotham JL.
[Negative intathoraic pressure decrees independently let ven
trculae filing and emptying. J Psiol 198),257120-H1SI,
54 Peters J. Kindred MK, Robotham JL. Transient analpss of car
‘iopulnionary intractions, I: diastolic event. Appl Psi
Ios 1306-1517,
55. Peters J, Kindred MK, Robotham JL. Transient analysis of car
iopulmionary intructions, H: systolic evens. J Appl Py
Iwaki TSI81528
56. Kitney RI. An ass of the nonlinear ehaior of the human
thermal vasomotor contol system. J Theor Biol. 197552:231-288,
57, Chess OF, Tam RM, Cale FR, Inlcace of eardite neural
‘pats on rhythmic variations of heart peri ithe ea. nt
Prose! 197522877578,
8, Sau JP, Kapian DT, Kitney RI. Now-inear interactions between
‘eepiraion and heait rae: a phenomenon common t malic
Plistlogc states I: Proc Cap in Cardio Lan Alaios,
(Cali: IEEE Computer Society Pres, 198815.29-802
Kitney RL, Rompelman O. Analysis of the interaction of th
human blGod pressure and thermal system, Ta Perkins J, od
‘Biomedical Computing. London, UK: Pitman Medical 19773054.
Peron PB, Biumann IE, Ehmke H, Nats B, Wittmann U,
Kircher HR, Phase and 2¢-h Mood presare conte by endo:
thclium-derved relaxing Taclor in conscios dogs. lm J Pio
ooo:26341 39511400
Dutrey-Dupagne C. Girard A, Uimana A, Elghosi JL. Etets of
the converting enzyme intortrandolapril on shor term va
tity of blood pressure in ental hypertension Clin Anon es
toot.
Mania G, Grassi G, Parti G, Daffonchio A. Evaluating sympa
het ati in hur hypertension J yperns. 199:11Guppl
S)s1si
68, Cohen FA, Hara K, Simpson G, Seon BM, Flora 3, Assessment
‘of sympathetic activation by lower body negative presure using
Spectral analysis of hear rate varatyand forearm ples
‘ography. Can J Cardiol. 1991-1 uppl A119
64, Kinet, Thompon IM, Kye HL MePheron GA, Seine,
Ir rate spectral analysis cardi nor
muscle smpathetie nerve activity daring
human sympathetic nerous setation and flare Cian
osm
Kicasle MG, Ferguson DW, Birkett CL, Myers GA, Berg W
Mariano J. Clinical. hemovynamic and sympathetic neural cor
relates of heart rate varity congestive heat fare. Am J
Canto 190:85°701-757
(66, Dalfoncio A, FranvelC, Di Rienzo M, Castigo P, Ramicer
‘A, Part G, Ferrars AU, Manca 6. Elle of sypatctony
‘ood pressure variably in the conscious rt. 7 Fypeaens, 19
soppy 70871
67. Adamopoulos S, Piepoll M. McCance A, Bernardi L, Rocadel A,
‘Ormerod 0. Siig P. Comparison of diferent methods (oF
‘sscaing sympathoragil Balance in chronic congestive, heat
Tallre secondary to coronary ortery diseass. Am Car. 1992;
sysask2
(68, Ponse J, Honzikowa N, Pisce B Spectalanahss of resting var
lyf some cculatory parameters in man Physiol Boke
torsr seas.
(9, Homzowa N, Bena J, Fier, tovidal features of circulatory
omer spoctra in man, Eur Appl Piya. 1939-30434,
Binkley PF, Haas Gd, Starling KC, Nunziata E,Hton PA, Leer
CV, Cosy RU, Sostained sgmeniation of parasympathetic tne
‘sith angtensn-convertingensyine inition in paints ith
‘ngestve heart failure. Jn Coll Cari. WAS21685-68,
‘anenes U. Physiologica interpretation of aulonpetra, coherence
“nu phase spetra of blood pressure, heart rat, and respiration
‘waves in man. uomedion, 172.1610,
72, Yougue BG, MeCabe PM, Porpes SW, Rivera M, Kelley SL.
Ackles PK. The effects of pharmacological manipulations thal
inflence vagal conte of the heart om heart peta, beat petal
acabiiy and respiration bn ras Pyehopiyslogs. 19219
202,
73, Hohnloser SH, Klingenichen T, Zabel M, Schroder F, Just HL
Intrainvidul ceproducibiity of heart rate variability. PACE.
982: part 2):2011 2315,
74, Cera €. Gastin MP, Paultre CZ, Lo M, Julien C, Vincent M,
‘Saar J, Autonomic nervous sytem and cardiovascular vai-
lity i eats seca analysts proach, mJ Pho, 19;
261-1292 H1289,
15, Lexy MN. Synpatti parasympathtie interactions inthe heart
Gi Ress WT BOTS
9
o
0
1
1286 Hypertension Vol 25, No 6 June 1995
76, Marin PJ, Lewy JR, Wesborg S, Levy MN. Phasic effets of
repetitive tag stimulation on arial contraction. Cre Res. 183;
5287-668,
77, Eekberp DL, Nethed C, Wallin BG. Respiratory modulation of
muscle sympatetie and vagal cardac outflow in man, J Pil
(Lond). 1988.65:18-196,
78, Mancka G, Mark AL. Arterial baroreflscs is humans. In:
‘Shepherd JT, Abboud FM, eds. Handbook of Physio, Section 2
The Cantiowaseular Stem Vole IN, Penpheral Cleation and
(Organ Blond Flow. Hetheus, Mas American Physiological Society,
WR 755-79,
79, Malig M, Camm AS. Components of heat rte vasabliy what
tho ay an and hat wy ewan J Cand
1095, 72821-802,
0, Novak V, Novak P, De Champlain J, Le Blane AR, Matin R.
Nadeau RInluence of respration’on heart rate and bod
pressure fictations. Appl Pil 1993;7:617-626,
si, Hineh JA, Bishop B. Respiratory snus arehythmis in humans
how breathing patern modulates heart rate. Am Physio
1981; 241 10.19,
82. Paraii G, Omboni S, Fratola A, Di Ricazo M, Zancheti A,
Manca G, Dynamic evaluation of the baroreflee in. ambulet
subjects Ia: Di Rieazo M, Mancia G, Para G, Pedot
Zanchetti A, eds. Blood Pressure and Heat Rate Varibiy,
“Amsterdam, Netherlands: 1OS Press, 1992:123-197
85. Di Rienzo MI, Bernie G, Cvallaa A, Ferrari AU, Pedoti A,
Manca G. Evaluation of arterial barorellen by analysis of the
‘ntroarteria (BP) recording. Ia: Dal Pall C, Pesioa A, eds
‘of Intemational Symposium on Ambutetoy Monitonns
(ISAM) Padova. Cleup. 1986:10-131
‘4, Herter G, Di Rienro M, Cavallarsi A, Ferrari AU, Pedot A,
Mancis ©. Evakstion of baroreepior telex by blood presure
‘monitoring in unanesthclized cals. Arm J Pipsiol. 1988;25%
TTS.
8S, PaatiG, Di Rienz0 M, BertinieriG, Pomidoss G, Casadei R,
Groppeli A, Pedott A, Zancet: A, Mancia G. Evaluation of the
bnroreceptor-heart rie reflex by 2thour intra-arterial blood
pressure monitoring in humans. fh
‘80, Pagani M. Somers V, Furlan R, Delf Oto 8, Convay J, Basel G,
‘Cerut§ SleightP, Malian A. Changes in autonomic regulation
induced by physical taining in ald hypertension. Hpenension,
198812:600610.
S57, Robbe HWS, Mulder LIM, Rude! H, Langewitz WA, Veldman
BP, Mulder G- Assessment of barorceptorrellex sensitivity by
‘means of spectral anaes. Hypertension. 198710838843,
88. Appel ML, Saul JP, Berger RD, Coen RJ. Cased-oop identi
‘ation of bio pressare variability mechan. In Di Rienan M,
Manes G, Para G, Pedoti A, Zanchet A eds. Blood Presure
and Hear’ Rate Variabiiy. Amsterdam, Nethctlands TOS Press
928876
89, Triedman JK, Saul JP. Blood pressure modulation by central
‘venous pressure and resiraon: bullering eects ofthe het ate
Fetlewes: Cvelion. 19689158179.
Berger RD, Saul JP, Coben RJ, Assessment of autonomic
response by broad-band respiration IEEE Trans Biomed En,
193036: 1061-10658,
1, Gazz S, Pacaluga E, Cast, Cerut S, Lombard, Pagani
M, Malini A” Sympathetic predominanes in escnialhyper-
tension: a stidy employing spectral anais of heart ate ari
ability. J Hypertens. 1986-7117.
Sus §, Johnson EH. Stress, autonomic hyperactivity and
‘sential hypertension: an enigma. J Hypertens. 1985:3(uppl 4):
i117.
93. Folkow B. Physiological agents of primary hypertension. sil
Rev, 1S22347-50,
94, ManciaG, Paral G. Reactivity to physia! and behavioural stress
tnd blod pressure variability ta bypertension Ie: lus, Bact
DR, eds. Handbook of Hiperension, Volume % Behavioural
Factors n Hypertension. Amsterdam, Netherlands: Elevier
Science Publishing: 1987: 104-122
95. Smyth HS, Sleight P, Pickering GW. Reflex regulation of arterial
pressure during sleepin man. Cire Res 1969,24:108-121
96, Imole BPM, Langewouters GJ, van Montfans GA, Prati, van
‘Goudoever J, Weseling Kit, Wing W, ManciaG. easily of
ambulatory, continuous 24-hour finger arterial pressure recording.
Hypertension. W9S215-73
97. ParatiG, Di Rienzo M, Ombori , Castioni P, Fratola A,
Mancia G. Spectral analysis of 2h blood pressure recordings. Am
LH ypertens. SASSI.
98, Wessling KH, de Wit B,Settels J, Klawe WH. On the indireet
‘eqitration of finger Mood pressure ater Pena. Bunt Bol Me
1980: 1.285-250,
98, Paral G, Cast R, Groppell A, Di Reno M, Mancis ©. Com-
rrhon f finger an inrarterl blod presare monterng re
fn ding laboratory testing. perio. 98960765,
10, OmboniS, Parti G, Fratola A, Mutt E, Di Rienzo M, Cation
P, Manca G. Spectral and sequence ‘analysis of finger blood
pressure variably: comparison with analsi of intra-arterial
Feeotdings. Hipeension. 195:222538
S-ar putea să vă placă și
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Actin-Myosin Complex and Implications For: Structure The Muscle ContractionDocument8 paginiActin-Myosin Complex and Implications For: Structure The Muscle ContractionBarış YaradanakulÎncă nu există evaluări
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- Actin-Myosin Complex and Implications For: Structure The Muscle ContractionDocument8 paginiActin-Myosin Complex and Implications For: Structure The Muscle ContractionBarış YaradanakulÎncă nu există evaluări
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- ReportDocument1 paginăReportBarış YaradanakulÎncă nu există evaluări
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (399)
- Rayment 1Document9 paginiRayment 1Barış YaradanakulÎncă nu există evaluări
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- A New Interpretation ofDocument12 paginiA New Interpretation ofBarış YaradanakulÎncă nu există evaluări
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Schematic Cross Section of A Metal-Oxide-Semiconductor Field-Effect Transistor (MOSFET)Document19 paginiSchematic Cross Section of A Metal-Oxide-Semiconductor Field-Effect Transistor (MOSFET)Barış YaradanakulÎncă nu există evaluări
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Deterministic Chaos Theory and Its Applications To Materials ScienceDocument9 paginiDeterministic Chaos Theory and Its Applications To Materials ScienceBarış YaradanakulÎncă nu există evaluări
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Multi-Scale Simulation of Nanoindentation On Cast Inconel 718 and NBCDocument10 paginiMulti-Scale Simulation of Nanoindentation On Cast Inconel 718 and NBCBarış YaradanakulÎncă nu există evaluări
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- 1 s2.0 S0927025615007272 MainDocument12 pagini1 s2.0 S0927025615007272 MainBarış YaradanakulÎncă nu există evaluări
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Adams - Calculus A Complete Course 7th c2010 - Student Solution ManualDocument354 paginiAdams - Calculus A Complete Course 7th c2010 - Student Solution ManualBarış Yaradanakul67% (3)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)