S-ar putea să vă placă și
- Sponsorship: Who's Eligible & How to ApplyDe la EverandSponsorship: Who's Eligible & How to ApplyÎncă nu există evaluări
- Health Guard: Proposal Form: Relationship Beyond InsuranceDocument2 paginiHealth Guard: Proposal Form: Relationship Beyond Insurancerajvansh katiyarÎncă nu există evaluări
- Criti Care PFDocument3 paginiCriti Care PFAlina Fatma0% (1)
- Health Statement FormDocument2 paginiHealth Statement FormRose Ann DuqueÎncă nu există evaluări
- Group Mediclaim Insurance-Proposal Form: Bajaj Allianz General Insurance Co. LTDDocument3 paginiGroup Mediclaim Insurance-Proposal Form: Bajaj Allianz General Insurance Co. LTDDenver SaldanhaÎncă nu există evaluări
- Premier Proposal 5f2bd12e92Document5 paginiPremier Proposal 5f2bd12e92bajaj enterprisesÎncă nu există evaluări
- Optima Restore Proposal Form OfflineDocument9 paginiOptima Restore Proposal Form OfflinemanohargudÎncă nu există evaluări
- Iob Health Care Plus Policy Proposal FormDocument2 paginiIob Health Care Plus Policy Proposal FormPritamjit RoutÎncă nu există evaluări
- HDFC ERGO General Insurance Company Limited: Easy Health - Proposal FormDocument8 paginiHDFC ERGO General Insurance Company Limited: Easy Health - Proposal FormDilip ManiyarÎncă nu există evaluări
- Future Vector Care-Proposal Form (Single Member)Document2 paginiFuture Vector Care-Proposal Form (Single Member)Arup GhoshÎncă nu există evaluări
- Saral Suraksha Bima, Plan - Preposal Form - v1Document3 paginiSaral Suraksha Bima, Plan - Preposal Form - v1rajeshÎncă nu există evaluări
- GEMI Application Form - Two Wheeler LoansDocument5 paginiGEMI Application Form - Two Wheeler LoansLuckyÎncă nu există evaluări
- Deed of Assignment - 102018Document5 paginiDeed of Assignment - 102018Kawaii YoshinoÎncă nu există evaluări
- Form 300 - Feb 2021Document13 paginiForm 300 - Feb 2021PREM MURUGANÎncă nu există evaluări
- Optima RestoreDocument6 paginiOptima RestoreYOGESH SHARMAÎncă nu există evaluări
- Member Enrolment Form-GTL-without Addendum-19 Nov 2018Document2 paginiMember Enrolment Form-GTL-without Addendum-19 Nov 2018Rajesh MukkavilliÎncă nu există evaluări
- National Insurance Varistha Proposal FormDocument5 paginiNational Insurance Varistha Proposal FormAnirBanerjee0% (1)
- PRP 23 7000179227PRP 23 7000179227Document7 paginiPRP 23 7000179227PRP 23 7000179227Arvind KumarÎncă nu există evaluări
- Application Form: Tata Aia Life Insurance Company LimitedDocument6 paginiApplication Form: Tata Aia Life Insurance Company LimitedpritamÎncă nu există evaluări
- Kutumb Swasthya Bima Policy - GroupDocument4 paginiKutumb Swasthya Bima Policy - Grouprohit kakkarÎncă nu există evaluări
- Form 300 March 2020Document12 paginiForm 300 March 2020shahnawazÎncă nu există evaluări
- Application For Individual Insurance FormDocument2 paginiApplication For Individual Insurance FormShenna RojasÎncă nu există evaluări
- Form 300 Revised 01-02-2020 PDFDocument11 paginiForm 300 Revised 01-02-2020 PDFAnuj VatsÎncă nu există evaluări
- Sukshma Hospi CashDocument4 paginiSukshma Hospi CashAdemuyiwa OlaniyiÎncă nu există evaluări
- LIC Health Plus Plan No.901 Full FormDocument15 paginiLIC Health Plus Plan No.901 Full FormDhaval SarvaiyaÎncă nu există evaluări
- Lic DocsDocument11 paginiLic DocsRahul ChauhanÎncă nu există evaluări
- Reliance Health Claim FormDocument4 paginiReliance Health Claim FormarijitnirmalÎncă nu există evaluări
- Colour Photo of The Life To Be AssuredDocument10 paginiColour Photo of The Life To Be AssuredRAKTIM PUJARIÎncă nu există evaluări
- Cancer Cover Proposal Form Revised 2023Document8 paginiCancer Cover Proposal Form Revised 2023Prasanth Vedgarb50% (2)
- Medicare Health Insurance Company LimitedDocument2 paginiMedicare Health Insurance Company LimitedVijay Singh ThakurÎncă nu există evaluări
- Ab Arogyadaan Proposal FormDocument2 paginiAb Arogyadaan Proposal FormMurthy0% (1)
- Health Guard Proposal Form PrintDocument4 paginiHealth Guard Proposal Form Printrock_on_rupz99Încă nu există evaluări
- Health Insurance Application FormDocument2 paginiHealth Insurance Application FormFrenzy Taher100% (1)
- Employee Enrollment Application: Group Size 51+ Eligible Employees - Medically UnderwrittenDocument6 paginiEmployee Enrollment Application: Group Size 51+ Eligible Employees - Medically Underwrittenmdugan5026Încă nu există evaluări
- Bjaz GC Policy ScheduleDocument5 paginiBjaz GC Policy ScheduleAbhishekÎncă nu există evaluări
- Enrolment Form - Group Credit Secure Plus: 1. Proposer'S InformationDocument2 paginiEnrolment Form - Group Credit Secure Plus: 1. Proposer'S Informationirfan shamaÎncă nu există evaluări
- Form 360 March 2020Document11 paginiForm 360 March 2020shahnawaz100% (1)
- Application For Reinstatement or Policy ChangeDocument2 paginiApplication For Reinstatement or Policy ChangeCristhelDelaTorreÎncă nu există evaluări
- MediCard Standard Plan FormDocument31 paginiMediCard Standard Plan FormCheskaPink TemonesÎncă nu există evaluări
- Reliancegeneral - Co.in 1800 3009 4890 3009: Health Claim FormDocument4 paginiReliancegeneral - Co.in 1800 3009 4890 3009: Health Claim FormSumit BhallaÎncă nu există evaluări
- Dental Reimbursement 2010Document6 paginiDental Reimbursement 2010marcelo galarzaÎncă nu există evaluări
- Claimants Statement Group Death Claim 05262021 Updated 1Document5 paginiClaimants Statement Group Death Claim 05262021 Updated 1JAIRUS DELOSREYESÎncă nu există evaluări
- Muthoot Finance Business Loan XH Enrolment Form v1Document2 paginiMuthoot Finance Business Loan XH Enrolment Form v1Subramanyam JonnaÎncă nu există evaluări
- (A Non-Linked Non-Participating Group Insurance Product) : Member Consent Form For ICICI Pru Super Protect CreditDocument2 pagini(A Non-Linked Non-Participating Group Insurance Product) : Member Consent Form For ICICI Pru Super Protect Creditvishu.dipu132Încă nu există evaluări
- Life Insurance Corporation of India IPR-F300-V1.0Document6 paginiLife Insurance Corporation of India IPR-F300-V1.0Rishikesh PrasadÎncă nu există evaluări
- Application Form Enwealth New AccountDocument2 paginiApplication Form Enwealth New AccounticttumainiÎncă nu există evaluări
- Bajaj Allianz My Home Insurance Proposal Form PDFDocument7 paginiBajaj Allianz My Home Insurance Proposal Form PDFMohamed IbrahimÎncă nu există evaluări
- 2024 Medicard IF Application FormDocument2 pagini2024 Medicard IF Application FormAlyzza EscalanteÎncă nu există evaluări
- IP Enrollment FormDocument2 paginiIP Enrollment FormSrigandh's WealthÎncă nu există evaluări
- UCO - GROUP CARE 360 APPLICATION FORM (Scheme For Customers of UCO Bank) (JULY-5th) - CompressedDocument2 paginiUCO - GROUP CARE 360 APPLICATION FORM (Scheme For Customers of UCO Bank) (JULY-5th) - CompressedRahulSinghÎncă nu există evaluări
- LVGI Policy ProposalDocument2 paginiLVGI Policy Proposals KollaÎncă nu există evaluări
- Life Insurance Beneficiary Designation Form - GeneraliDocument2 paginiLife Insurance Beneficiary Designation Form - Generalijohn gerald reynoÎncă nu există evaluări
- Health Claim Form: Part A (To Be Filled by Insured)Document3 paginiHealth Claim Form: Part A (To Be Filled by Insured)Harshad DhodiÎncă nu există evaluări
- SUNLIFEDocument2 paginiSUNLIFEGiacenÎncă nu există evaluări
- Proposal Form 906 Aarogya RakshakDocument22 paginiProposal Form 906 Aarogya RakshakBharath Kumar K83% (6)
- 2022 Individual Tax Organizer FillableDocument6 pagini2022 Individual Tax Organizer FillableTham DangÎncă nu există evaluări
- Proposal Form Niveshplus and SiipDocument13 paginiProposal Form Niveshplus and Siipsidhulic76Încă nu există evaluări
- Mediprime: Claim FormDocument4 paginiMediprime: Claim FormMunna Bhai MbaÎncă nu există evaluări
- Proposal Form: Flexi HealthDocument5 paginiProposal Form: Flexi HealthSANDEEP familyÎncă nu există evaluări
- Ap421fe 0216B NDDocument3 paginiAp421fe 0216B NDDen NisÎncă nu există evaluări
- Eczema (Dermatitis), Atopic Dermatitis, Seborrhoeic DermatitisDocument25 paginiEczema (Dermatitis), Atopic Dermatitis, Seborrhoeic DermatitisAtqiya Maisha LataÎncă nu există evaluări
- Clinical Features, Evaluation, and Diagnosis of Sepsis in Term and Late Preterm Infants PDFDocument27 paginiClinical Features, Evaluation, and Diagnosis of Sepsis in Term and Late Preterm Infants PDFJonathan WelchÎncă nu există evaluări
- An Avenue of Assessing Towards Preventive Actions of The Local Government Unit of Tanza, Cavite Response To COVID - 19 PandemicDocument2 paginiAn Avenue of Assessing Towards Preventive Actions of The Local Government Unit of Tanza, Cavite Response To COVID - 19 Pandemicjetlee estacionÎncă nu există evaluări
- Gems and Astrology - Gemstones AstrologyDocument5 paginiGems and Astrology - Gemstones Astrologykrishan_lokhande100% (1)
- CHN ExamDocument21 paginiCHN ExamExemplar ReviewÎncă nu există evaluări
- AntacidsDocument5 paginiAntacidsRowela Mae LibradillaÎncă nu există evaluări
- Active and Passive ImmunityDocument68 paginiActive and Passive Immunityintan100% (2)
- About The Series - Read MeDocument4 paginiAbout The Series - Read MejlhotaruÎncă nu există evaluări
- Philippine Integrated Disease Surveillance and Response (Pidsr) "PIDSR A Bedrock of Effective Disease Surveillance" - Secretary DuqueDocument4 paginiPhilippine Integrated Disease Surveillance and Response (Pidsr) "PIDSR A Bedrock of Effective Disease Surveillance" - Secretary DuqueRoel AbricaÎncă nu există evaluări
- Daftar PustakaDocument2 paginiDaftar PustakaYuli ErmaÎncă nu există evaluări
- Vaginal InfectionsDocument2 paginiVaginal InfectionsIndhumathiÎncă nu există evaluări
- D&D 5e SkavenDocument1 paginăD&D 5e SkavensyÎncă nu există evaluări
- Thermostatic Mixing Valves Type Operation PDFDocument28 paginiThermostatic Mixing Valves Type Operation PDFSlobodanÎncă nu există evaluări
- Comparison of Goldmann Applanation Tonometer, Tono-PenDocument19 paginiComparison of Goldmann Applanation Tonometer, Tono-PenLidiasilambaÎncă nu există evaluări
- Title Group B Streptococcal Infection in Non-Pregnant AdultsDocument17 paginiTitle Group B Streptococcal Infection in Non-Pregnant AdultsHam FGÎncă nu există evaluări
- Zika (1) InfografiaDocument2 paginiZika (1) Infografiaandrea lula da silvaÎncă nu există evaluări
- Coronavirus Politics: The Comparative Politics and Policy of Covid-19Document663 paginiCoronavirus Politics: The Comparative Politics and Policy of Covid-19Conceição Lemes100% (2)
- Tetratology Hand OutsDocument1 paginăTetratology Hand OutsAngielyn Montibon JesusÎncă nu există evaluări
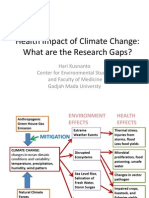
- 2 - Prof Hari Kusnanto - Climate Change and Impacts On Health in IndonesiaDocument12 pagini2 - Prof Hari Kusnanto - Climate Change and Impacts On Health in IndonesiaMohammad Rahman HakimÎncă nu există evaluări
- Approach To Pleural EffusionDocument46 paginiApproach To Pleural EffusionBaskoro Tri LaksonoÎncă nu există evaluări
- Impact of Covid-19Document9 paginiImpact of Covid-19adane yehualawÎncă nu există evaluări
- Diarrhea NCPDocument34 paginiDiarrhea NCPchezian smartÎncă nu există evaluări
- KayachikitsaDocument14 paginiKayachikitsasivva1986Încă nu există evaluări
- Yellow Fever FactsDocument2 paginiYellow Fever FactsFactPalooza100% (1)
- Population GrowthDocument13 paginiPopulation GrowthManel MamitooÎncă nu există evaluări
- Disease Diagnosis System: Software Requirement Specification (SRS)Document11 paginiDisease Diagnosis System: Software Requirement Specification (SRS)Shubham BhadauriaÎncă nu există evaluări
- Streptokinase GroupDocument16 paginiStreptokinase GroupSuffocated LiveÎncă nu există evaluări
- Domestic Rabbits Diseases and ParasitesDocument31 paginiDomestic Rabbits Diseases and ParasitesAlvaro Pauchard Pino100% (1)
- Pa 1 Persuasive EssayDocument4 paginiPa 1 Persuasive Essayapi-458023500Încă nu există evaluări
- Skoda Corretto Barley Glucans Obesity08Document2 paginiSkoda Corretto Barley Glucans Obesity08bcs002Încă nu există evaluări