S-ar putea să vă placă și
- Orthoptic Exercises for OptometristsDocument6 paginiOrthoptic Exercises for OptometristsCatalin GeorgeÎncă nu există evaluări
- Neil H. Riordan - Stem Cell Therapy A Rising Tide How Stem Cells Are Disrupting Medicine and Transforming LivesDocument341 paginiNeil H. Riordan - Stem Cell Therapy A Rising Tide How Stem Cells Are Disrupting Medicine and Transforming LivesLuca Dato100% (2)
- Ocular Anatomy - The RetinaDocument106 paginiOcular Anatomy - The RetinaJaneÎncă nu există evaluări
- Adult Cataract: Cortical or Soft CataractDocument6 paginiAdult Cataract: Cortical or Soft CataractJohn Christopher LucesÎncă nu există evaluări
- Keratometer Easy To Understand PDFDocument2 paginiKeratometer Easy To Understand PDFDanielle SangalangÎncă nu există evaluări
- Module 5 - Ocular Motility - Cover TestDocument12 paginiModule 5 - Ocular Motility - Cover TestCat Loved KirariÎncă nu există evaluări
- Pediatric Eye Examination: Seia MahananiDocument35 paginiPediatric Eye Examination: Seia MahananiRaissaÎncă nu există evaluări
- The GlaucomasDocument29 paginiThe GlaucomasJk FloresÎncă nu există evaluări
- Clinical Orthoptics - Fiona Rowe - 146Document6 paginiClinical Orthoptics - Fiona Rowe - 146Danielle SangalangÎncă nu există evaluări
- Binocular Vision Anomalies: Symptomatic HeterophoriaDocument10 paginiBinocular Vision Anomalies: Symptomatic HeterophoriaGraham CoffeyÎncă nu există evaluări
- Retinal AnatomyDocument86 paginiRetinal AnatomySean ScogginsÎncă nu există evaluări
- Anatomy of the Uvea: Iris, Ciliary Body and ChoroidDocument48 paginiAnatomy of the Uvea: Iris, Ciliary Body and ChoroidBinu AshrafÎncă nu există evaluări
- RETINOSCOPY: A KEY TO ASSESSING REFRACTIVE ERRORSDocument33 paginiRETINOSCOPY: A KEY TO ASSESSING REFRACTIVE ERRORSSafa Abdualrahaman Ali HamadÎncă nu există evaluări
- Pediatric Ophthalmology Anatomy and ExaminationDocument21 paginiPediatric Ophthalmology Anatomy and ExaminationGlydenne GayamÎncă nu există evaluări
- Degenerative MyopiaDocument53 paginiDegenerative MyopiaNiloy BasakÎncă nu există evaluări
- Clinical OpticsDocument88 paginiClinical OpticsKris ArchibaldÎncă nu există evaluări
- Incomitant SquintDocument41 paginiIncomitant Squintshreeja maheshwari100% (3)
- Lecture Three Convergence and Accommodation (AC/A) : Mr. Natnael L. (Lecturer) April/2017Document33 paginiLecture Three Convergence and Accommodation (AC/A) : Mr. Natnael L. (Lecturer) April/2017henok birukÎncă nu există evaluări
- The Spotty RetinaDocument5 paginiThe Spotty RetinaJose Luis Mato AhcanÎncă nu există evaluări
- Nungki-Esodeviations & ExodeviationsDocument36 paginiNungki-Esodeviations & ExodeviationsNia RoosdhantiaÎncă nu există evaluări
- Neonatal ResuscitationDocument15 paginiNeonatal Resuscitationpriyanka88% (8)
- Refraction and AccommodationDocument80 paginiRefraction and Accommodationapi-19916399100% (2)
- Basic Eye ExamDocument8 paginiBasic Eye ExamLisa AguilarÎncă nu există evaluări
- Colour Vision AnomaliesDocument27 paginiColour Vision AnomaliesGershon HayfordÎncă nu există evaluări
- Mental Health ProgramDocument33 paginiMental Health ProgramjosephÎncă nu există evaluări
- No. 11 JEBSENS MARITIME v. JESSIE D. ALCIBARDocument3 paginiNo. 11 JEBSENS MARITIME v. JESSIE D. ALCIBARnhizza dawn Daligdig100% (1)
- Blurring of Vision Ii: Retinal Vascular Disorders: Dr. Jose BondocDocument15 paginiBlurring of Vision Ii: Retinal Vascular Disorders: Dr. Jose BondocRea Dominique CabanillaÎncă nu există evaluări
- Objective Refraction Technique: Retinoscopy: Aao ReadingDocument57 paginiObjective Refraction Technique: Retinoscopy: Aao ReadingKhairunnisaÎncă nu există evaluări
- Congenital Strabismus: S. Vanitha, B.optom, 3 YearDocument23 paginiCongenital Strabismus: S. Vanitha, B.optom, 3 YearDivya Priya Dharmalingam100% (1)
- Low Vision: Assessment and Educational Needs: A Guide to Teachers and ParentsDe la EverandLow Vision: Assessment and Educational Needs: A Guide to Teachers and ParentsÎncă nu există evaluări
- Visual Field InterpretationsDocument35 paginiVisual Field InterpretationsAhmadhassan RanaÎncă nu există evaluări
- KERATOCONUSDocument22 paginiKERATOCONUSAarush DeoraÎncă nu există evaluări
- RGP Fitting +++++Document18 paginiRGP Fitting +++++Philip McNelsonÎncă nu există evaluări
- KeratometryDocument3 paginiKeratometrycarol_marie_3Încă nu există evaluări
- Retinal Detachment SlideDocument54 paginiRetinal Detachment SlideHerin NataliaÎncă nu există evaluări
- College of Medicine and Health Science, Department of OptometryDocument47 paginiCollege of Medicine and Health Science, Department of Optometryhenok birukÎncă nu există evaluări
- Binocular vision anomalies overviewDocument13 paginiBinocular vision anomalies overviewblueiceÎncă nu există evaluări
- Third Years Log BookDocument11 paginiThird Years Log BookMeenakshi Kumar100% (2)
- 12 - Objective RefractionDocument11 pagini12 - Objective RefractionSumon SarkarÎncă nu există evaluări
- Ophthalmology Board Review Notes: Intermediate and Posterior UveitisDocument12 paginiOphthalmology Board Review Notes: Intermediate and Posterior Uveitissharu4291Încă nu există evaluări
- Hey, Doc! What’S Wrong with My Eye?: A General Guide to Eye SymptomsDe la EverandHey, Doc! What’S Wrong with My Eye?: A General Guide to Eye SymptomsÎncă nu există evaluări
- Trabeculectomy Complications: Characteristics and ManagementDocument31 paginiTrabeculectomy Complications: Characteristics and ManagementalfarizyjefryÎncă nu există evaluări
- MCQ 05 OpticsDocument14 paginiMCQ 05 OpticsAmr Abdulradi0% (1)
- Cycloplegic Refraction in Optometric Practice 1337594763401 2Document14 paginiCycloplegic Refraction in Optometric Practice 1337594763401 2Strauss de LangeÎncă nu există evaluări
- Paediatric Optometry Part 1 exam answersDocument5 paginiPaediatric Optometry Part 1 exam answersSourav KarmakarÎncă nu există evaluări
- Prevent Pests in Under 40Document6 paginiPrevent Pests in Under 40Shima Fariza50% (2)
- AAO GoniosDocument43 paginiAAO GoniosmeliabudiÎncă nu există evaluări
- Module+2+nursing+Document82 paginiModule+2+nursing+Dyah AnggrainiÎncă nu există evaluări
- Eye Docs RetinaDocument279 paginiEye Docs RetinaRahul LokhandeÎncă nu există evaluări
- Cycloplegic Retinoscopy in InfancyDocument5 paginiCycloplegic Retinoscopy in InfancyStrauss de LangeÎncă nu există evaluări
- Corneal Cross-Linking: Treatment for Cornea DiseaseDe la EverandCorneal Cross-Linking: Treatment for Cornea DiseaseÎncă nu există evaluări
- Strabismus Quick GuideDocument4 paginiStrabismus Quick Guideghitza80100% (1)
- New Anatomy and Physiology of MaculaDocument51 paginiNew Anatomy and Physiology of MaculaPragnya Rao Donthineni75% (4)
- Case Studies PresbyopiaDocument33 paginiCase Studies PresbyopiaMalaika ZubairÎncă nu există evaluări
- Refractive Errors & Refractive SurgeryDocument97 paginiRefractive Errors & Refractive SurgeryDr-Fadi AlkayyaliÎncă nu există evaluări
- RefraksiDocument84 paginiRefraksinaroetocapkutilÎncă nu există evaluări
- Direct OphthalmoscopeDocument16 paginiDirect OphthalmoscopeMuhammed AbdulmajeedÎncă nu există evaluări
- Fundus ExaminationDocument43 paginiFundus Examinationsamuelpnrj25100% (2)
- Lens and CataractDocument55 paginiLens and CataractRold Brio Sos100% (1)
- AniseikoniaDocument40 paginiAniseikoniahenok biruk100% (1)
- Mechanisms of Cataract Formation: Nicholas Phelps Brown MD, FRCS, FrcophthDocument7 paginiMechanisms of Cataract Formation: Nicholas Phelps Brown MD, FRCS, FrcophthQomariah RiaÎncă nu există evaluări
- Development of Binocular Vision: University of Gondar Department of Optometry by Nebiyat FelekeDocument35 paginiDevelopment of Binocular Vision: University of Gondar Department of Optometry by Nebiyat Felekehenok birukÎncă nu există evaluări
- PUCAN, Julienne BSN III-D - SGD - HYPO&HYPERCHLOREMIADocument10 paginiPUCAN, Julienne BSN III-D - SGD - HYPO&HYPERCHLOREMIAJulienne PucanÎncă nu există evaluări
- 0.1 Chapter 7 - Ethical Considerations On Community Health NursingDocument45 pagini0.1 Chapter 7 - Ethical Considerations On Community Health NursingyounggirldavidÎncă nu există evaluări
- AHA ASA-AV Malformation 2017Document25 paginiAHA ASA-AV Malformation 2017Kym DominguezÎncă nu există evaluări
- OrthoticsDocument37 paginiOrthoticsergosadia658Încă nu există evaluări
- JETIR1905867 - Reduction in Drug Dosage - DR - BiswaroopRoyChowdhury PDFDocument12 paginiJETIR1905867 - Reduction in Drug Dosage - DR - BiswaroopRoyChowdhury PDFSudhir YadavÎncă nu există evaluări
- Buy Adderall 5 MG OnlineDocument11 paginiBuy Adderall 5 MG OnlineAdderall UsaÎncă nu există evaluări
- NMES Electrode Placement GuideDocument2 paginiNMES Electrode Placement GuideSkye EllisÎncă nu există evaluări
- How I Assess and Manage The Risk of Bleeding in Patients Treated For Venous ThromboembolismDocument11 paginiHow I Assess and Manage The Risk of Bleeding in Patients Treated For Venous ThromboembolismHugo HectorÎncă nu există evaluări
- Isk IiDocument70 paginiIsk IikafhcompÎncă nu există evaluări
- Aplastic Anaemia: DR Sandeep M R Physician Jayanagar General Hospial BangaloreDocument26 paginiAplastic Anaemia: DR Sandeep M R Physician Jayanagar General Hospial BangaloreSandeep m rÎncă nu există evaluări
- Minnesota Department of Health Decision TreeDocument5 paginiMinnesota Department of Health Decision TreeDuluth News TribuneÎncă nu există evaluări
- Mobile Guide Antenatal CareDocument11 paginiMobile Guide Antenatal CarePearlwhyte BrownÎncă nu există evaluări
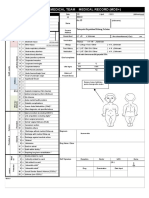
- Emergency Medical Team Medical Record (MDS+) : MDS - Check All That ApplyDocument2 paginiEmergency Medical Team Medical Record (MDS+) : MDS - Check All That ApplySyafiraIdhatunNasyiahÎncă nu există evaluări
- Pediatric Red Ear Syndrome: A Case Report of An Erythromelalgia Type and Review of The LiteratureDocument4 paginiPediatric Red Ear Syndrome: A Case Report of An Erythromelalgia Type and Review of The LiteraturedanniwebbÎncă nu există evaluări
- BIOL 5200 Final Review GuideDocument18 paginiBIOL 5200 Final Review GuideClaudia Ann RutlandÎncă nu există evaluări
- 267 Impulses Serving Pain Sensation in The Left Foot Are RelayedDocument12 pagini267 Impulses Serving Pain Sensation in The Left Foot Are RelayedNathanÎncă nu există evaluări
- Commission+Meeting+Public+Comment March+25,+2020 20.15 PDFDocument9 paginiCommission+Meeting+Public+Comment March+25,+2020 20.15 PDFal_crespoÎncă nu există evaluări
- Clinical cariology and operative dentistry in the 21st centuryDocument4 paginiClinical cariology and operative dentistry in the 21st centuryDavid MonroyÎncă nu există evaluări
- Human Oral FunctionDocument12 paginiHuman Oral FunctionGondoriyo PkmÎncă nu există evaluări
- Fungal InfectionsDocument29 paginiFungal InfectionsKaran MassÎncă nu există evaluări
- Severe Sepsis-Associated Morbidity and Mortality Among Critically Ill Children With CancerDocument8 paginiSevere Sepsis-Associated Morbidity and Mortality Among Critically Ill Children With CancerFaki D'pasnizerÎncă nu există evaluări
- DNA VIRUSES-handout PDFDocument11 paginiDNA VIRUSES-handout PDFROTHESSA MARY CARINGALÎncă nu există evaluări
- Psychiartry NotesDocument38 paginiPsychiartry NotesAlthea Lujille PinazoÎncă nu există evaluări
- Legalizing Marijuana in The PhilippinesDocument15 paginiLegalizing Marijuana in The PhilippinesEnzo MacTavish SendohÎncă nu există evaluări