S-ar putea să vă placă și
- Infusion Therapy TrainingDocument19 paginiInfusion Therapy Trainingjeremie cruz100% (1)
- Manual for Iv Therapy Procedures & Pain Management: Fourth EditionDe la EverandManual for Iv Therapy Procedures & Pain Management: Fourth EditionÎncă nu există evaluări
- Safety Injectables WorkbookDocument110 paginiSafety Injectables Workbookgeraffe94% (17)
- Quality ImprovementDocument18 paginiQuality ImprovementEka AdiputraÎncă nu există evaluări
- Primary Urgent Care Guidelines UtiDocument22 paginiPrimary Urgent Care Guidelines UtiUti Nilam SariÎncă nu există evaluări
- Smart Meter Are HarmfulDocument165 paginiSmart Meter Are HarmfulknownpersonÎncă nu există evaluări
- Checklist Patient SafetyDocument15 paginiChecklist Patient SafetyKatherine Conlu Bengan100% (1)
- Running Head: NURSING STANDARDS 1Document20 paginiRunning Head: NURSING STANDARDS 1api-253509573Încă nu există evaluări
- Pathophysiology of AtherosclerosisDocument27 paginiPathophysiology of AtherosclerosisAmira Paguyo QuilapioÎncă nu există evaluări
- Muster List: Vessel: M/T "Stena President" Call Sign: ZCDR6 Master: YURIY YASHINDocument9 paginiMuster List: Vessel: M/T "Stena President" Call Sign: ZCDR6 Master: YURIY YASHINwwaallÎncă nu există evaluări
- 325 WHO Surgical Safety ChecklistDocument8 pagini325 WHO Surgical Safety ChecklistAlfie YannurÎncă nu există evaluări
- PUD QuestionsDocument5 paginiPUD QuestionsAmira Paguyo QuilapioÎncă nu există evaluări
- Series 90 100cc Pump Parts ManualDocument152 paginiSeries 90 100cc Pump Parts ManualHernan Garcia67% (3)
- Using Patient Reported Outcomes to Improve Health CareDe la EverandUsing Patient Reported Outcomes to Improve Health CareÎncă nu există evaluări
- A Job InterviewDocument8 paginiA Job Interviewa.rodriguezmarcoÎncă nu există evaluări
- Evidenced Based Nursing PracticeDocument7 paginiEvidenced Based Nursing PracticeKim ViñasÎncă nu există evaluări
- Civil Law 1Document2 paginiCivil Law 1Len Sor Lu100% (3)
- Adult Nasogastric Tube Insertion Procedure & Management PolicyDocument0 paginiAdult Nasogastric Tube Insertion Procedure & Management PolicyRubelyn Joy LazarteÎncă nu există evaluări
- Project Proposal On Improving QualityDocument4 paginiProject Proposal On Improving Qualityzakuan79100% (2)
- Np2 AnswerDocument13 paginiNp2 AnswerMarie Jhoana100% (1)
- 1 A Synopsis of IVT in The PhilippinesDocument17 pagini1 A Synopsis of IVT in The PhilippinesPrince Rener Velasco PeraÎncă nu există evaluări
- PDS Air CompressorDocument1 paginăPDS Air Compressordhavalesh1Încă nu există evaluări
- Quality Improvement Paper FinalDocument11 paginiQuality Improvement Paper Finalapi-291740538Încă nu există evaluări
- Journal Article Critique Nursing 665Document5 paginiJournal Article Critique Nursing 665api-214213767Încă nu există evaluări
- Safety ChecklistDocument8 paginiSafety ChecklistdharmaÎncă nu există evaluări
- Evidence-Based Nursing PracticeDocument12 paginiEvidence-Based Nursing PracticeJaylen Cay100% (6)
- FNCP Improper DrainageDocument3 paginiFNCP Improper DrainageAmira Paguyo Quilapio50% (2)
- Critical Pathway: Clinical Pathways Have Four Main Components (Hill, 1994, Hill 1998)Document5 paginiCritical Pathway: Clinical Pathways Have Four Main Components (Hill, 1994, Hill 1998)pooja singhÎncă nu există evaluări
- Ebp PaperDocument8 paginiEbp Paperapi-250304529Încă nu există evaluări
- Applying Lean Principles To Reduce Wait Times in A VA Emergency DepartmentDocument10 paginiApplying Lean Principles To Reduce Wait Times in A VA Emergency DepartmentNida KhoiriahÎncă nu există evaluări
- Literature Review On Surgical Safety ChecklistDocument11 paginiLiterature Review On Surgical Safety Checklistfut0mipujeg3100% (1)
- Quality and Safety Synthesis PaperDocument6 paginiQuality and Safety Synthesis Paperapi-252807964Încă nu există evaluări
- Development and Implementation of A Clinical Pathway Programme in An Acute Care General Hospital in SingaporeDocument10 paginiDevelopment and Implementation of A Clinical Pathway Programme in An Acute Care General Hospital in SingaporeAisyah ShofiÎncă nu există evaluări
- Nurs490 Safety Performance Improvement Paper Neuburg IntroDocument2 paginiNurs490 Safety Performance Improvement Paper Neuburg Introapi-452041818Încă nu există evaluări
- C C The Problem and Its BackgroundDocument7 paginiC C The Problem and Its BackgroundKristine CustodioÎncă nu există evaluări
- Accurate Assessment of Patient Weight - Nursing TimesDocument7 paginiAccurate Assessment of Patient Weight - Nursing TimesDani PhilipÎncă nu există evaluări
- QI Student Proposal Handoffs PDFDocument6 paginiQI Student Proposal Handoffs PDFDxtr MedinaÎncă nu există evaluări
- Question of Acute CareDocument11 paginiQuestion of Acute CareKuberAiranÎncă nu există evaluări
- Ebp Project 5 FinalDocument6 paginiEbp Project 5 Finalapi-315880679Încă nu există evaluări
- Leadership Paper 2-Revised-1Document9 paginiLeadership Paper 2-Revised-1api-237668254Încă nu există evaluări
- Apss VapDocument14 paginiApss VapRoxanA BocaÎncă nu există evaluări
- CQI by CommitteeDocument6 paginiCQI by CommitteeJhOy XiÎncă nu există evaluări
- Ignatavicius: Medical-Surgical Nursing, 7th EditionDocument9 paginiIgnatavicius: Medical-Surgical Nursing, 7th EditionGERALDE CHARLESÎncă nu există evaluări
- The Positive Impact of Continuous ImprovementDocument15 paginiThe Positive Impact of Continuous ImprovementMane DaralÎncă nu există evaluări
- Injectable Artesunate Field Testing ReportDocument33 paginiInjectable Artesunate Field Testing ReportmlutfimaÎncă nu există evaluări
- Managing Healthcare QualityDocument7 paginiManaging Healthcare QualityTooba SiddiquiÎncă nu există evaluări
- Bedside Handover PDFDocument20 paginiBedside Handover PDFshutekiÎncă nu există evaluări
- Dr. Ashraf Ismail PresentationDocument85 paginiDr. Ashraf Ismail PresentationBudi YunantoÎncă nu există evaluări
- Module1 SDLDocument88 paginiModule1 SDLbillboggins100% (1)
- Evidence-Based Quality Improvement Project For Determining - Gallant and Schultz - EBN - BMJ - 2005Document2 paginiEvidence-Based Quality Improvement Project For Determining - Gallant and Schultz - EBN - BMJ - 2005pareshÎncă nu există evaluări
- Phillips Postanaesthetic 2013Document11 paginiPhillips Postanaesthetic 2013Alex PiecesÎncă nu există evaluări
- Journal of Continuing Education in Nursing. 40 (5) :221-7, 2009 MayDocument10 paginiJournal of Continuing Education in Nursing. 40 (5) :221-7, 2009 MayJessica GabejanÎncă nu există evaluări
- Accepted Manuscript: Seminars in PerinatologyDocument10 paginiAccepted Manuscript: Seminars in PerinatologyAlberto Kenyo Riofrio PalaciosÎncă nu există evaluări
- Mathematical Modelling in Health Care: Karnon, J., Mark Mackay and T.M. MillsDocument13 paginiMathematical Modelling in Health Care: Karnon, J., Mark Mackay and T.M. MillsTyas AgustinaÎncă nu există evaluări
- Creating A Guide For Float NursesDocument1 paginăCreating A Guide For Float NursesJhouleen Angelika TamÎncă nu există evaluări
- Quality Improvement and Revalidation Two Goals, SDocument4 paginiQuality Improvement and Revalidation Two Goals, SRENAULTÎncă nu există evaluări
- A Protocol For The Management of Adhesive Small.2Document9 paginiA Protocol For The Management of Adhesive Small.2ktktkt01Încă nu există evaluări
- Informatics ProjectDocument7 paginiInformatics ProjectShannon TerrellÎncă nu există evaluări
- Quality and Safety Synthesis PaperDocument6 paginiQuality and Safety Synthesis Paperapi-260053520Încă nu există evaluări
- Clinical Indicator PDFDocument5 paginiClinical Indicator PDFTri Hastuti HendrayaniÎncă nu există evaluări
- Relationshipbasedcarepaper - NSG 4040-1Document13 paginiRelationshipbasedcarepaper - NSG 4040-1api-314231356Încă nu există evaluări
- Change ProjectDocument10 paginiChange ProjectMartin ManaluÎncă nu există evaluări
- Nursing Audit in Obstetric Care (1) - Mrs. Sarla TakooDocument45 paginiNursing Audit in Obstetric Care (1) - Mrs. Sarla TakooSaritaÎncă nu există evaluări
- Hourly Rounding and The Effects On Patient Safety and Satisfaction ArtifactDocument29 paginiHourly Rounding and The Effects On Patient Safety and Satisfaction Artifactapi-310375757Încă nu există evaluări
- 7051N3M126Q411U7Document69 pagini7051N3M126Q411U7naldihasibuanÎncă nu există evaluări
- 5 Storyboard (Contoh 1)Document1 pagină5 Storyboard (Contoh 1)RaniCianTarÎncă nu există evaluări
- Hospitalists and Their Impact On Quality, Patient Safety, and SatisfactionDocument14 paginiHospitalists and Their Impact On Quality, Patient Safety, and SatisfactionNurunnisa yrÎncă nu există evaluări
- Tammy Tarner Journal Club EntryDocument1 paginăTammy Tarner Journal Club Entryapi-357707616Încă nu există evaluări
- Qiproposalpaper HartbargerDocument6 paginiQiproposalpaper Hartbargerapi-427611602Încă nu există evaluări
- Chapter 017Document15 paginiChapter 017dtheart2821100% (2)
- 20 Ways To Use Social Media For Social GoodDocument2 pagini20 Ways To Use Social Media For Social GoodAmira Paguyo QuilapioÎncă nu există evaluări
- How To Avoid Online ScamsDocument4 paginiHow To Avoid Online ScamsAmira Paguyo QuilapioÎncă nu există evaluări
- RDO No. 6 - Urdaneta City, East PangasinanDocument671 paginiRDO No. 6 - Urdaneta City, East PangasinanAmira Paguyo QuilapioÎncă nu există evaluări
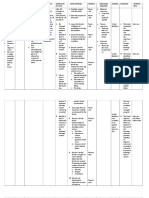
- Generic Name Brand Name Classification Dosage Mechanism of Action Indication Contraindication Side Effects Nursing ImplicationDocument2 paginiGeneric Name Brand Name Classification Dosage Mechanism of Action Indication Contraindication Side Effects Nursing ImplicationAmira Paguyo QuilapioÎncă nu există evaluări
- TungsDocument2 paginiTungsAmira Paguyo QuilapioÎncă nu există evaluări
- Health Problem Family Nursing Problem Goal of Care Specific Objective of Care Nursing Intervention Methods OF Contact Resources Required EvaluationDocument1 paginăHealth Problem Family Nursing Problem Goal of Care Specific Objective of Care Nursing Intervention Methods OF Contact Resources Required EvaluationAmira Paguyo QuilapioÎncă nu există evaluări
- School of Nursing Saint Louis University: RD Title (Midterms) Total Score ScoreDocument1 paginăSchool of Nursing Saint Louis University: RD Title (Midterms) Total Score ScoreAmira Paguyo QuilapioÎncă nu există evaluări
- Saint Louis University: School of NursingDocument1 paginăSaint Louis University: School of NursingAmira Paguyo QuilapioÎncă nu există evaluări
- The Foods, Supplements & Oils To Increase Bone Healing: NutritionDocument3 paginiThe Foods, Supplements & Oils To Increase Bone Healing: NutritionAmira Paguyo QuilapioÎncă nu există evaluări
- Epidural Flow ChartDocument1 paginăEpidural Flow ChartAmira Paguyo QuilapioÎncă nu există evaluări
- 1 Conflict in NG - Report - 28FEB2018Document46 pagini1 Conflict in NG - Report - 28FEB2018KrishnaÎncă nu există evaluări
- Branch CodeDocument3 paginiBranch CodeAhir MukherjeeÎncă nu există evaluări
- Software Test ISO StandardsDocument2 paginiSoftware Test ISO StandardsTony DavisÎncă nu există evaluări
- VM PDFDocument4 paginiVM PDFTembre Rueda RaúlÎncă nu există evaluări
- Uncertainty-Based Production Scheduling in Open Pit Mining: R. Dimitrakopoulos and S. RamazanDocument7 paginiUncertainty-Based Production Scheduling in Open Pit Mining: R. Dimitrakopoulos and S. RamazanClaudio AballayÎncă nu există evaluări
- Why Is Inventory Turnover Important?: ... It Measures How Hard Your Inventory Investment Is WorkingDocument6 paginiWhy Is Inventory Turnover Important?: ... It Measures How Hard Your Inventory Investment Is WorkingabhiÎncă nu există evaluări
- Vigi Module Selection PDFDocument1 paginăVigi Module Selection PDFrt1973Încă nu există evaluări
- Research On The Marketing Communication Strategy of Tesla Motors in China Under The Background of New MediaDocument5 paginiResearch On The Marketing Communication Strategy of Tesla Motors in China Under The Background of New MediaSiddharth ChaudharyÎncă nu există evaluări
- Paper - 1: Principles & Practice of Accounting Questions True and FalseDocument29 paginiPaper - 1: Principles & Practice of Accounting Questions True and FalsePiyush GoyalÎncă nu există evaluări
- ScriptDocument7 paginiScriptAllen Delacruz100% (1)
- Goal of The Firm PDFDocument4 paginiGoal of The Firm PDFSandyÎncă nu există evaluări
- Bank Soal LettersDocument17 paginiBank Soal Lettersderoo_wahidahÎncă nu există evaluări
- Raport de Incercare TL 82 Engleza 2015 MasticDocument3 paginiRaport de Incercare TL 82 Engleza 2015 MasticRoxana IoanaÎncă nu există evaluări
- Bill FormatDocument7 paginiBill FormatJay Rupchandani100% (1)
- Termsconditions of JionetDocument3 paginiTermsconditions of JionetskÎncă nu există evaluări
- J 2022 SCC OnLine SC 864 Tushardubey Symlaweduin 20221015 214803 1 23Document23 paginiJ 2022 SCC OnLine SC 864 Tushardubey Symlaweduin 20221015 214803 1 23Tushar DubeyÎncă nu există evaluări
- Mannitol For Reduce IOPDocument7 paginiMannitol For Reduce IOPHerryantoThomassawaÎncă nu există evaluări
- Centaur Profile PDFDocument5 paginiCentaur Profile PDFChandra MohanÎncă nu există evaluări
- Aaa0030imb02 FDocument30 paginiAaa0030imb02 FJvr Omar EspinozaÎncă nu există evaluări
- Arab Open University B326: Advanced Financial Accounting TMA - Spring 2022-2023 V2Document7 paginiArab Open University B326: Advanced Financial Accounting TMA - Spring 2022-2023 V2samiaÎncă nu există evaluări
- Service Bulletin: Service Bulletin NUMBER: 8.8/134A Caterpillar: Confidential Green Page 1 of 8Document8 paginiService Bulletin: Service Bulletin NUMBER: 8.8/134A Caterpillar: Confidential Green Page 1 of 8GutsavoÎncă nu există evaluări
- U HalliburtonDocument3 paginiU Halliburtonanas soufÎncă nu există evaluări
- Buffett Wisdom On CorrectionsDocument2 paginiBuffett Wisdom On CorrectionsChrisÎncă nu există evaluări