S-ar putea să vă placă și
- A Three Stage Approach To Full Mouth RehabilitationDocument10 paginiA Three Stage Approach To Full Mouth RehabilitationShyam K MaharjanÎncă nu există evaluări
- Braking MechanicsDocument55 paginiBraking MechanicsDyna AbhilashÎncă nu există evaluări
- Aging Facial Skeleton PrsDocument10 paginiAging Facial Skeleton PrsJorge TreviñoÎncă nu există evaluări
- Impression Techniques in Removable Partial DentureDocument8 paginiImpression Techniques in Removable Partial DentureLama Nahed100% (2)
- Vertical Maxillary ExcessDocument125 paginiVertical Maxillary ExcessYuvashreeÎncă nu există evaluări
- Development and Eruption of The TeethDocument5 paginiDevelopment and Eruption of The TeethZHAREIGHNEILE C. MAMOLOÎncă nu există evaluări
- GROWTH ASSESSMENT METHODSDocument65 paginiGROWTH ASSESSMENT METHODSdr parveen bathlaÎncă nu există evaluări
- MARPE AbdAllah BahaaDocument90 paginiMARPE AbdAllah BahaaOmar AbodoniaÎncă nu există evaluări
- Oral Surgery, Oral Diagnosis, Roentgenology: B. A Radiolucent Halo Surrounding The Root of The FractureDocument49 paginiOral Surgery, Oral Diagnosis, Roentgenology: B. A Radiolucent Halo Surrounding The Root of The FractureRC Dome100% (1)
- Diagnosis of Transverse Problems - 2019 - Seminars in Orthodontics PDFDocument8 paginiDiagnosis of Transverse Problems - 2019 - Seminars in Orthodontics PDFOmy J. CruzÎncă nu există evaluări
- Cervical Vertebrae MaturationDocument8 paginiCervical Vertebrae MaturationDavid DongÎncă nu există evaluări
- Diagnostic Aids in ProsthodonticsDocument60 paginiDiagnostic Aids in ProsthodonticsAME DENTAL COLLEGE RAICHUR, KARNATAKAÎncă nu există evaluări
- Single Complete DentureDocument70 paginiSingle Complete DentureKarthik KannaiyanÎncă nu există evaluări
- CVM McnamaraDocument11 paginiCVM McnamaraXnb HajiÎncă nu există evaluări
- 3.prediction of Mandibular Growth Rotation - Bj+ÂrkDocument11 pagini3.prediction of Mandibular Growth Rotation - Bj+ÂrkLudovica CoppolaÎncă nu există evaluări
- Darwis2 03 PDFDocument6 paginiDarwis2 03 PDFFelipe Maldonado ArayaÎncă nu există evaluări
- RDENJ - Volume 6 - Issue 2 - Pages 98-105Document8 paginiRDENJ - Volume 6 - Issue 2 - Pages 98-105Abdur RehmanÎncă nu există evaluări
- Mandibular Growth During Early ChildhoodDocument9 paginiMandibular Growth During Early ChildhoodmariaÎncă nu există evaluări
- Geometric Morphometric Analysis of Growth Patterns Among Facial TypesDocument12 paginiGeometric Morphometric Analysis of Growth Patterns Among Facial TypesFaridah RisnawatiÎncă nu există evaluări
- ReDocument3 paginiReIBARRA POLANIA MARIA JOSEÎncă nu există evaluări
- 2014 Sharma Age Changes of Jaws and Soft Tissue Profile HighlightedDocument8 pagini2014 Sharma Age Changes of Jaws and Soft Tissue Profile HighlightedHabeeb AL-AbsiÎncă nu există evaluări
- Longitudinal Changes in Facial GrowthDocument14 paginiLongitudinal Changes in Facial GrowthSrishti SyalÎncă nu există evaluări
- Differences Between Male and Female Mandibular Length Growth According To Panoramic RadiographDocument7 paginiDifferences Between Male and Female Mandibular Length Growth According To Panoramic Radiographyuni madjidÎncă nu există evaluări
- Ocr 12457Document7 paginiOcr 12457Rolando Huaman BravoÎncă nu există evaluări
- Growth Patterns in Subjects With Long and Short FacesDocument12 paginiGrowth Patterns in Subjects With Long and Short FacesMatt SanoudosÎncă nu există evaluări
- SIO 2012 - Transverse Growth of Maxilla and MandibleDocument18 paginiSIO 2012 - Transverse Growth of Maxilla and MandibleGeorge JoseÎncă nu există evaluări
- International Journal of Trend in Scientific Research and Development (IJTSRD)Document8 paginiInternational Journal of Trend in Scientific Research and Development (IJTSRD)Editor IJTSRDÎncă nu există evaluări
- Arch Length Changes from Infancy to Mid-AdulthoodDocument6 paginiArch Length Changes from Infancy to Mid-AdulthoodLiceth Herrera MartinezÎncă nu există evaluări
- BBRC13 040Document8 paginiBBRC13 040Anonymous nyga3gm3Încă nu există evaluări
- The Frontal Sinus and N Andibutar Growth PredictionDocument5 paginiThe Frontal Sinus and N Andibutar Growth PredictionsmritiÎncă nu există evaluări
- A.M. Et Al. - 2014 - Agreement Between Cranial and Facial Classification Through Clinical Observation and Anthropometric Measurement AmoDocument8 paginiA.M. Et Al. - 2014 - Agreement Between Cranial and Facial Classification Through Clinical Observation and Anthropometric Measurement AmoDaniel Eduardo Jara RodríguezÎncă nu există evaluări
- Pileski Relacion Hueso SesamoideoDocument9 paginiPileski Relacion Hueso SesamoideoNico A Ore LudeÎncă nu există evaluări
- Maxillary Growth and Maturation During Infancy and Early ChildhoodDocument9 paginiMaxillary Growth and Maturation During Infancy and Early ChildhoodThendral DevanathanÎncă nu există evaluări
- Agradoc391 Testicular PDFDocument6 paginiAgradoc391 Testicular PDFClaudia IrimieÎncă nu există evaluări
- Tweed's philosophy and diagnostic facial triangleDocument9 paginiTweed's philosophy and diagnostic facial triangleManisha PillaiÎncă nu există evaluări
- Prediction of The Age of Maximum Puberal Growth in Body HeightDocument11 paginiPrediction of The Age of Maximum Puberal Growth in Body HeightNico A Ore LudeÎncă nu există evaluări
- The Aging Craniofacial Complex AJO-DO 2008Document10 paginiThe Aging Craniofacial Complex AJO-DO 2008Patricia BurbanoÎncă nu există evaluări
- Growth Changes in The Soft Tissue Facial ProfileDocument34 paginiGrowth Changes in The Soft Tissue Facial Profiledeepika jegatheesanÎncă nu există evaluări
- Dentofacial Growth Changes in Subjects With Untreated Class II Malocclusion From Late Puberty Through Young AdulthoodDocument7 paginiDentofacial Growth Changes in Subjects With Untreated Class II Malocclusion From Late Puberty Through Young AdulthoodSischa RamadhaniÎncă nu există evaluări
- SKELETAL AND DENTAL MATURITYDocument0 paginiSKELETAL AND DENTAL MATURITYdr parveen bathlaÎncă nu există evaluări
- Key Words: Frontal Sinus Development Age Estimation JuvenileDocument9 paginiKey Words: Frontal Sinus Development Age Estimation JuvenilefebriÎncă nu există evaluări
- Reliability of Growth Prediction With Hand - Wrist RadiographsDocument5 paginiReliability of Growth Prediction With Hand - Wrist Radiographscalmua1234Încă nu există evaluări
- Carlson DS - Transverse Development of The Human Jaws Between The Ages of 8.5 and 15.5 Years Studied Longitudinally With Use of ImplantsDocument11 paginiCarlson DS - Transverse Development of The Human Jaws Between The Ages of 8.5 and 15.5 Years Studied Longitudinally With Use of Implantscruzjulio480Încă nu există evaluări
- Evaluation of Mandibular First Molars' Axial Inclination and Alveolar Morphology in Different Facial Patterns: A CBCT StudyDocument10 paginiEvaluation of Mandibular First Molars' Axial Inclination and Alveolar Morphology in Different Facial Patterns: A CBCT StudyPututu PatataÎncă nu există evaluări
- Testing Standard Methods of Dental Age Estimation PDFDocument10 paginiTesting Standard Methods of Dental Age Estimation PDFAmira IzzatusyuhadaÎncă nu există evaluări
- Acta Odontol Scand. 2019 - 77 2 107-113Document8 paginiActa Odontol Scand. 2019 - 77 2 107-113Denise RodsevichÎncă nu există evaluări
- Treatment Timing For Rapid Maxillary ExpansionDocument8 paginiTreatment Timing For Rapid Maxillary Expansiongriffone1Încă nu există evaluări
- Bishara 1989Document14 paginiBishara 1989habeebÎncă nu există evaluări
- Craniofacial Growth, Maturation, and Change: Teens To MidadulthoodDocument4 paginiCraniofacial Growth, Maturation, and Change: Teens To MidadulthoodOmar DSÎncă nu există evaluări
- A Longitudinal Analysis of The Growth of Limb Segments in AdolescenceDocument11 paginiA Longitudinal Analysis of The Growth of Limb Segments in AdolescencerkonÎncă nu există evaluări
- Ferreira 2020Document10 paginiFerreira 2020Dela MedinaÎncă nu există evaluări
- Growth of The Anterior Dental Arch in Black American ChildrenDocument9 paginiGrowth of The Anterior Dental Arch in Black American ChildrennoxleekÎncă nu există evaluări
- Morphometric Analysis of Three Normal Facial Types in Mixed Dentition Using Posteroanterior Cephalometric Radiographs: Preliminary ResultsDocument6 paginiMorphometric Analysis of Three Normal Facial Types in Mixed Dentition Using Posteroanterior Cephalometric Radiographs: Preliminary ResultsSEBASTIAN ANDRES MIRANDA GONZALEZÎncă nu există evaluări
- Maxillary Tooth Width vs Facial DimensionsDocument7 paginiMaxillary Tooth Width vs Facial DimensionsVi LinhÎncă nu există evaluări
- Tweed's Philosophy-A Review: June 2018Document10 paginiTweed's Philosophy-A Review: June 2018rohitÎncă nu există evaluări
- Comparison of Airway Dimensions in Skeletal Class I PDFDocument8 paginiComparison of Airway Dimensions in Skeletal Class I PDFSoe San KyawÎncă nu există evaluări
- Association Between Overbite and Craniofacial Growth PatternDocument9 paginiAssociation Between Overbite and Craniofacial Growth PatternAriadna MéndezÎncă nu există evaluări
- Estadio de NollaDocument13 paginiEstadio de NollaCATALINA VASQUEZ LOPEZ100% (1)
- 424-Article Text-1272-1-11-20170906Document13 pagini424-Article Text-1272-1-11-20170906Ortodoncia UNAL 2020Încă nu există evaluări
- Comparacion Crecimiento Facial Clase I y Clase II BaccettiDocument7 paginiComparacion Crecimiento Facial Clase I y Clase II BaccettiPatricia BurbanoÎncă nu există evaluări
- Bishara - Changes in Facial DimensionsDocument15 paginiBishara - Changes in Facial Dimensionsosama nasserÎncă nu există evaluări
- Facial Soft TisuesDocument6 paginiFacial Soft TisuesMoni Garcia SantosÎncă nu există evaluări
- Dimensi Vertikal FotoDocument10 paginiDimensi Vertikal FotoPrevita NindaÎncă nu există evaluări
- Growth Charts For Nose Length, Nasal Protrusion, and Philtrum Length From Birth To 97 YearsDocument4 paginiGrowth Charts For Nose Length, Nasal Protrusion, and Philtrum Length From Birth To 97 Yearssoumalya481Încă nu există evaluări
- Adenoids and Diseased Tonsils: Their Effect on General IntelligenceDe la EverandAdenoids and Diseased Tonsils: Their Effect on General IntelligenceÎncă nu există evaluări
- Evo-Devo of Child Growth: Treatise on Child Growth and Human EvolutionDe la EverandEvo-Devo of Child Growth: Treatise on Child Growth and Human EvolutionÎncă nu există evaluări
- Brain Tumors in ChildrenDe la EverandBrain Tumors in ChildrenAmar GajjarÎncă nu există evaluări
- Denture Trouble Shooting GuideDocument5 paginiDenture Trouble Shooting Guideairtifa1Încă nu există evaluări
- Classification and Sequelae of Arrested Eruption of Primary MolarsDocument7 paginiClassification and Sequelae of Arrested Eruption of Primary MolarsRisana RahoofÎncă nu există evaluări
- Interocclusal RecordsDocument8 paginiInterocclusal RecordsJohnÎncă nu există evaluări
- Magnitude of Clearance in The Anterior Region and Displacement After Complete Denture InsertionDocument16 paginiMagnitude of Clearance in The Anterior Region and Displacement After Complete Denture InsertionJames LinÎncă nu există evaluări
- Operator Position, Visibility, Illumination, and Finger RestDocument14 paginiOperator Position, Visibility, Illumination, and Finger RestjihanÎncă nu există evaluări
- English PPT Eka Ok Respon Periodontal Terhadap Kekuatan Dari LuarDocument32 paginiEnglish PPT Eka Ok Respon Periodontal Terhadap Kekuatan Dari LuarNexelsÎncă nu există evaluări
- Errors Associated With Digital Preview of Computer-Engineered Complete Dentures and Guidelines For Reducing Them: A Technique ArticleDocument11 paginiErrors Associated With Digital Preview of Computer-Engineered Complete Dentures and Guidelines For Reducing Them: A Technique ArticletovarichÎncă nu există evaluări
- Oral Habits and Its Relationship To Malocclusion A Review.20141212083000Document4 paginiOral Habits and Its Relationship To Malocclusion A Review.20141212083000Stacia AnastashaÎncă nu există evaluări
- (03241750 - Acta Medica Bulgarica) Computer Program for Digital Data Analysis of Facebow Records - Part ІIDocument6 pagini(03241750 - Acta Medica Bulgarica) Computer Program for Digital Data Analysis of Facebow Records - Part ІITeodorÎncă nu există evaluări
- Oclusion, Guia Canina Revision Bibliografica, 2007Document13 paginiOclusion, Guia Canina Revision Bibliografica, 2007MiguelÎncă nu există evaluări
- Articulo 1 PDFDocument9 paginiArticulo 1 PDFJURY CASTRO PINEDAÎncă nu există evaluări
- The Third Point of Reference and Its Effect On The Protrusive Condylar Guidance Angles Obtained in Semi-Adjustable ArticulatorDocument7 paginiThe Third Point of Reference and Its Effect On The Protrusive Condylar Guidance Angles Obtained in Semi-Adjustable Articulatorayush srivastavaÎncă nu există evaluări
- Classification of MalocclusionDocument79 paginiClassification of MalocclusionMittali Vaibhav Sabnis50% (2)
- Interdisciplinary Approach To The MandibDocument7 paginiInterdisciplinary Approach To The MandibZachary DuongÎncă nu există evaluări
- A Simplified Approach For Restoration of Worn Dentition Using The Full MockDocument10 paginiA Simplified Approach For Restoration of Worn Dentition Using The Full MockHaCem SahbaniÎncă nu există evaluări
- Fixed Prosthodontics I - Lecture 1 - Glossary of ProsthodonticsDocument6 paginiFixed Prosthodontics I - Lecture 1 - Glossary of ProsthodonticsNoor Al-Deen Maher100% (1)
- CJT 041Document8 paginiCJT 041Nada EmadÎncă nu există evaluări
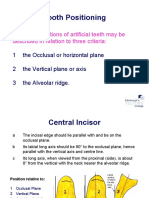
- Tooth Positioning: The Basic Positions of Artificial Teeth May Be Described in Relation To Three CriteriaDocument19 paginiTooth Positioning: The Basic Positions of Artificial Teeth May Be Described in Relation To Three CriteriaCherine SnookÎncă nu există evaluări
- Recent Advances in Provisional RestorationsDocument6 paginiRecent Advances in Provisional RestorationsAngelia PratiwiÎncă nu există evaluări
- Ajuste Oclusal de OcclusionMadeEasy PreviewDocument7 paginiAjuste Oclusal de OcclusionMadeEasy PreviewrichcristalÎncă nu există evaluări
- MCQ 15 Sample Questions PDFDocument4 paginiMCQ 15 Sample Questions PDFغمدان دماج الحمزيÎncă nu există evaluări
- Course Specification OcclusionDocument5 paginiCourse Specification OcclusionamrsheblksÎncă nu există evaluări
- Boltons AnalysisDocument23 paginiBoltons Analysiswidhariyani purnomoputriÎncă nu există evaluări