S-ar putea să vă placă și
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- UNISCO Price Proposal FormatDocument3 paginiUNISCO Price Proposal Formatchoclate2012Încă nu există evaluări
- Installation ListsDocument1 paginăInstallation Listschoclate2012Încă nu există evaluări
- Section 1 - Instructions To Bidders: Table of ClausesDocument22 paginiSection 1 - Instructions To Bidders: Table of Clauseschoclate2012Încă nu există evaluări
- Request For Expressions of Interest (Consulting Services - Firms Selection)Document2 paginiRequest For Expressions of Interest (Consulting Services - Firms Selection)choclate2012Încă nu există evaluări
- Completed Projects 2017 1Document2 paginiCompleted Projects 2017 1choclate2012Încă nu există evaluări
- RTPI Briefing NotesDocument4 paginiRTPI Briefing Noteschoclate2012Încă nu există evaluări
- Mechanical, Electrical and PLubmbing SOW PDFDocument25 paginiMechanical, Electrical and PLubmbing SOW PDFchoclate2012Încă nu există evaluări
- Civil WorksDocument6 paginiCivil Workschoclate2012100% (1)
- Company Fact Sheet PDFDocument27 paginiCompany Fact Sheet PDFchoclate2012Încă nu există evaluări
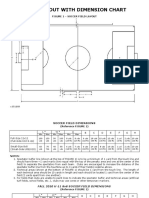
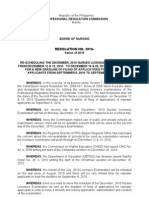
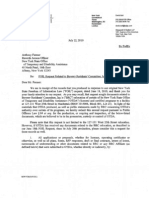
- 11v11 Soccer Field DimensionsDocument2 pagini11v11 Soccer Field Dimensionschoclate2012Încă nu există evaluări
- 6th Central Pay Commission Salary CalculatorDocument15 pagini6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- Big City Plan - Work in Progress Doucment 2008 PDFDocument84 paginiBig City Plan - Work in Progress Doucment 2008 PDFchoclate2012Încă nu există evaluări
- Sports FieldDocument48 paginiSports Fieldchoclate2012Încă nu există evaluări
- LawGuide2013 PDFDocument32 paginiLawGuide2013 PDFchoclate2012Încă nu există evaluări
- Parkinson Report - BCP Visioning Study PDFDocument80 paginiParkinson Report - BCP Visioning Study PDFchoclate2012Încă nu există evaluări
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5795)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1091)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Thesis 2Document69 paginiThesis 2Christine Gaerlan100% (1)
- !indx SaepDocument3 pagini!indx SaepHamid Ali JoyiaÎncă nu există evaluări
- 6.-Organic-Resource-Agency-v4-170915-AH-food Waste in ScotlandDocument27 pagini6.-Organic-Resource-Agency-v4-170915-AH-food Waste in ScotlandVita NurhikmahÎncă nu există evaluări
- PRC-BON Resolution No. 17 Series of 2010Document2 paginiPRC-BON Resolution No. 17 Series of 2010PhilippineNursingDirectory.comÎncă nu există evaluări
- NauliDocument2 paginiNauliGurjit Singh BoparaiÎncă nu există evaluări
- Altered Parent Infant NCP PDFDocument3 paginiAltered Parent Infant NCP PDFAebee AlcarazÎncă nu există evaluări
- Coronavirus Disease (COVID-19) : Philippine National Police Health Service PNP General HospitalDocument1 paginăCoronavirus Disease (COVID-19) : Philippine National Police Health Service PNP General HospitalKarsenley Cal-el Iddig BurigsayÎncă nu există evaluări
- 015 Barium ChlorideDocument7 pagini015 Barium Chlorideeng20072007Încă nu există evaluări
- Soal Semester Genap Kelas X 2019Document7 paginiSoal Semester Genap Kelas X 2019Aris SulistyoÎncă nu există evaluări
- PacmakerDocument37 paginiPacmakerSalman HabeebÎncă nu există evaluări
- Kertas Trial English Perlis K1 Set B 2021Document13 paginiKertas Trial English Perlis K1 Set B 2021darwish erfanÎncă nu există evaluări
- Flex Built PT2 PDFDocument2 paginiFlex Built PT2 PDFPedro Augusto100% (4)
- Students' Nutrition - School Canteen Affecting Their Food ChoiceDocument19 paginiStudents' Nutrition - School Canteen Affecting Their Food ChoicesamantaÎncă nu există evaluări
- Black SwanDocument1 paginăBlack Swan3D - AURELIO, Lyca Mae M.Încă nu există evaluări
- 1st Decision - G.R. No. 217872Document11 pagini1st Decision - G.R. No. 217872MerÎncă nu există evaluări
- Chaos, Solitons and Fractals: Vinay Kumar Reddy Chimmula, Lei ZhangDocument6 paginiChaos, Solitons and Fractals: Vinay Kumar Reddy Chimmula, Lei ZhangS AbdÎncă nu există evaluări
- Subdermal HematomaDocument2 paginiSubdermal HematomaDristi KhanalÎncă nu există evaluări
- Rewire Your BrainDocument0 paginiRewire Your BrainJohn Bates100% (1)
- Easy-Stop Trailer ABS: Maintenance Manual No. 33 Revised 4-98Document44 paginiEasy-Stop Trailer ABS: Maintenance Manual No. 33 Revised 4-98VNMaroccoÎncă nu există evaluări
- Moleskine Wellness Template PDFDocument13 paginiMoleskine Wellness Template PDFFolinÎncă nu există evaluări
- Pondicherry School Education RulesDocument17 paginiPondicherry School Education RulesAr Ramya Prasad0% (1)
- Speech SkincareDocument2 paginiSpeech SkincarePI40621 Fatin Alyaa Binti Abdullah ZawawiÎncă nu există evaluări
- R.A 9710 - Magna Carta For WomenDocument15 paginiR.A 9710 - Magna Carta For WomenFrances Ann TevesÎncă nu există evaluări
- My New and Improved ResumeDocument3 paginiMy New and Improved Resumeapi-281905332Încă nu există evaluări
- Research Paper OutlineDocument3 paginiResearch Paper Outlineapi-317142831Încă nu există evaluări
- LP U1209300 Inoa 2013 Inoa Color ChartDocument4 paginiLP U1209300 Inoa 2013 Inoa Color ChartbinreÎncă nu există evaluări
- Otda Foil Request 2Document4 paginiOtda Foil Request 2sammyschwartz08Încă nu există evaluări
- Hotel and Room Facilities (Part3g1)Document14 paginiHotel and Room Facilities (Part3g1)Mary Joy CelamorÎncă nu există evaluări
- Yes We CanDocument3 paginiYes We CanSpeech & Language Therapy in PracticeÎncă nu există evaluări
- Self-Esteem Moderates The Associations Between Body-Related Self-Conscious Emotions and Depressive SymptomsDocument11 paginiSelf-Esteem Moderates The Associations Between Body-Related Self-Conscious Emotions and Depressive SymptomsAlliyah Roma CadaÎncă nu există evaluări