S-ar putea să vă placă și
- Diaphragmatic HerniaDocument8 paginiDiaphragmatic HerniaAnonymous 9xHTwHYÎncă nu există evaluări
- Memory SkillsDocument70 paginiMemory SkillsAsiri Samanatha Elegoda100% (1)
- Sensory Processing and Autism Evidence Research Future Directions DR Roseann Schaaf PDFDocument59 paginiSensory Processing and Autism Evidence Research Future Directions DR Roseann Schaaf PDFKiyorÎncă nu există evaluări
- Enteral Nutrition in The Critically Ill Marik PDFDocument8 paginiEnteral Nutrition in The Critically Ill Marik PDFCami Cuevas VergaraÎncă nu există evaluări
- UNIT-5 Pharmacology of NeurosurgeryDocument12 paginiUNIT-5 Pharmacology of NeurosurgeryFaizan Mazhar100% (1)
- Guidelines For The Management of Severe Traumatic Brain Injury 4th EditionDocument62 paginiGuidelines For The Management of Severe Traumatic Brain Injury 4th EditionNailahRahmahÎncă nu există evaluări
- Nursing Care of The Patient With Neurological DisordersDocument89 paginiNursing Care of The Patient With Neurological DisordersRaveenmayiÎncă nu există evaluări
- gbs4 171105053149Document71 paginigbs4 171105053149Theresia Avila KurniaÎncă nu există evaluări
- AppendicitisDocument11 paginiAppendicitisbobtagubaÎncă nu există evaluări
- Reflexology - 5 Power PointsDocument6 paginiReflexology - 5 Power Pointsrickiti9100% (1)
- Traumatic Brain InjuryDocument23 paginiTraumatic Brain InjuryRisal WintokoÎncă nu există evaluări
- Thyroid Function TestDocument11 paginiThyroid Function TestBookmyscansÎncă nu există evaluări
- Increased ICPDocument7 paginiIncreased ICPK-La BreanneÎncă nu există evaluări
- Principles of Opioid Management: Symptom GuidelinesDocument45 paginiPrinciples of Opioid Management: Symptom GuidelinesTheresia Avila KurniaÎncă nu există evaluări
- Aubrey de Grey - SENSDocument57 paginiAubrey de Grey - SENSBruceKlein50% (2)
- CarePlans PDFDocument130 paginiCarePlans PDFTheresia Avila KurniaÎncă nu există evaluări
- Ishihara Colour Plates - 38 Set GuideDocument13 paginiIshihara Colour Plates - 38 Set Guidenelutza_popÎncă nu există evaluări
- Brain Injury Resuscitation 2009Document8 paginiBrain Injury Resuscitation 2009Dandy Azmi AzwirÎncă nu există evaluări
- Pathophysiology and Management of ICH and Brain Hypoxia After TBIDocument13 paginiPathophysiology and Management of ICH and Brain Hypoxia After TBIitalofgÎncă nu există evaluări
- Morning Case DiscussionDocument21 paginiMorning Case Discussionسلطان الحنبصيÎncă nu există evaluări
- Intracerebral Hemorrhage Medical TreatmentDocument3 paginiIntracerebral Hemorrhage Medical TreatmentDarrel Allan MandiasÎncă nu există evaluări
- Critical AppraisalDocument15 paginiCritical AppraisalRio HerawanÎncă nu există evaluări
- Critical Care of Patients With Acute Ischemic and Hemorrhagic StrokeDocument7 paginiCritical Care of Patients With Acute Ischemic and Hemorrhagic StrokeMary Jhane VillanuevaÎncă nu există evaluări
- Helbok 2018Document3 paginiHelbok 2018Julieta PereyraÎncă nu există evaluări
- New Therapies For Intracranial Hypertension: Review ArticleDocument10 paginiNew Therapies For Intracranial Hypertension: Review ArticleBeny RiliantoÎncă nu există evaluări
- Ebp Head Up 30Document9 paginiEbp Head Up 30La fazaÎncă nu există evaluări
- 12 JMSCRDocument6 pagini12 JMSCRArdianÎncă nu există evaluări
- JURNAL Sip 1Document30 paginiJURNAL Sip 1Irwan SabriÎncă nu există evaluări
- MannitolDocument10 paginiMannitolFenzy Septiana AnggrainiÎncă nu există evaluări
- Emergency Airway Management in The Patient With Elevated ICP UpToDateDocument16 paginiEmergency Airway Management in The Patient With Elevated ICP UpToDateJoyce CarolineÎncă nu există evaluări
- Bansal 2021 - Neutral Spinal Compress HRVDocument2 paginiBansal 2021 - Neutral Spinal Compress HRVdudekula salmaÎncă nu există evaluări
- Management of Raised Intracranial Pressure in Children With Traumatic Brain Injury - PMCDocument19 paginiManagement of Raised Intracranial Pressure in Children With Traumatic Brain Injury - PMChadi40canadaÎncă nu există evaluări
- Management of raised intracranial pressure in childrenDocument24 paginiManagement of raised intracranial pressure in childrenMita AmaliaÎncă nu există evaluări
- Nihms687466 PDFDocument14 paginiNihms687466 PDFyoiiiÎncă nu există evaluări
- Tiopentone Vs PentobarbitalDocument10 paginiTiopentone Vs PentobarbitalFrank PuchiÎncă nu există evaluări
- Effect of Early Physiotherapy On Intracranial PressureDocument6 paginiEffect of Early Physiotherapy On Intracranial Pressurebendot29Încă nu există evaluări
- Management of Moderate To Severe Traumatic Brain Injury 2022Document18 paginiManagement of Moderate To Severe Traumatic Brain Injury 2022Vladimir BasurtoÎncă nu există evaluări
- Guidelines For Management EspañolDocument14 paginiGuidelines For Management EspañolGrace KellyÎncă nu există evaluări
- Current Concepts and Advancements in TBIDocument3 paginiCurrent Concepts and Advancements in TBIMacros FitÎncă nu există evaluări
- Brainhypoxiaisassociatedwithshort Termoutcomeafterseveretraumaticbraininjuryindependentlyofi 2Document9 paginiBrainhypoxiaisassociatedwithshort Termoutcomeafterseveretraumaticbraininjuryindependentlyofi 2indahÎncă nu există evaluări
- Head Injury Management: Ahimbisibwe Alaphael Lecturer DR - JulietDocument33 paginiHead Injury Management: Ahimbisibwe Alaphael Lecturer DR - JulietNinaÎncă nu există evaluări
- Oddo 2009Document6 paginiOddo 2009rodolfo riosÎncă nu există evaluări
- Use of Hyperoncotic Human Albumin Solution in Severe Traumatic Brain Injury Revisited-A Narrative Review and Meta-AnalysisDocument10 paginiUse of Hyperoncotic Human Albumin Solution in Severe Traumatic Brain Injury Revisited-A Narrative Review and Meta-Analysisjose luis iribarrenÎncă nu există evaluări
- Managing Increased Intracranial PressureDocument13 paginiManaging Increased Intracranial PressureLudmila PirtacÎncă nu există evaluări
- Tugas Bu EltrikaDocument20 paginiTugas Bu EltrikaHervina22Încă nu există evaluări
- Intracranial Pressure: Presenter: NailaDocument26 paginiIntracranial Pressure: Presenter: NailaInam KhanÎncă nu există evaluări
- Cerebral Perfusion PressureDocument36 paginiCerebral Perfusion PressureAbdullah Shidqul AzmiÎncă nu există evaluări
- The Coagulation DefectDocument9 paginiThe Coagulation DefectTimotius Wira YudhaÎncă nu există evaluări
- B5W2 - Brainstem Herniation TreatmentDocument2 paginiB5W2 - Brainstem Herniation TreatmentCatherine MernaÎncă nu există evaluări
- Management of Acute Severe Traumatic Brain InjuryDocument19 paginiManagement of Acute Severe Traumatic Brain InjuryMustafa AadanÎncă nu există evaluări
- Evaluation and Management of Elevated Intracranial Pressure in Adults - UpToDateDocument41 paginiEvaluation and Management of Elevated Intracranial Pressure in Adults - UpToDateManuelEduardoSanchezSotoÎncă nu există evaluări
- 2.-Management of Moderate To Severe Traumatic Brain Injury An Update For The IntensivistDocument18 pagini2.-Management of Moderate To Severe Traumatic Brain Injury An Update For The IntensivistEllys Macías PeraltaÎncă nu există evaluări
- Hypertension: SMF Saraf Rsud Bangli Fakultas Kedokteran Universitas Islam Al-Azhar 2018Document49 paginiHypertension: SMF Saraf Rsud Bangli Fakultas Kedokteran Universitas Islam Al-Azhar 2018Muhammad HidayatullahÎncă nu există evaluări
- Title: Sildenafil in The The Management of Patients With SevereDocument2 paginiTitle: Sildenafil in The The Management of Patients With SevereAnca Oprea TighiliuÎncă nu există evaluări
- Surgical Management: SurgeryDocument5 paginiSurgical Management: SurgeryKarl Angelo MontanoÎncă nu există evaluări
- Increased Intracranial Pressure - StatPearls - NCBI BookshelfDocument5 paginiIncreased Intracranial Pressure - StatPearls - NCBI BookshelfWIWI HRÎncă nu există evaluări
- Stroke 2013 Qureshi S67 9Document4 paginiStroke 2013 Qureshi S67 9Herlinda Dwi NingrumÎncă nu există evaluări
- Ventilatory Strategies For Patients With Acute Brain InjuryDocument8 paginiVentilatory Strategies For Patients With Acute Brain InjuryKhalid Walid AhmadÎncă nu există evaluări
- Focused Management of Patients With Severe Acute Brain Injury and ARDSDocument12 paginiFocused Management of Patients With Severe Acute Brain Injury and ARDSPepeee:DÎncă nu există evaluări
- Management Head Injury in ICUDocument5 paginiManagement Head Injury in ICUIrma KusumaÎncă nu există evaluări
- JNNB 4 144Document4 paginiJNNB 4 144luciaÎncă nu există evaluări
- Wolfe-Management of Intracranial Pressure-Curr Neurol Neurosci Rep-2009Document9 paginiWolfe-Management of Intracranial Pressure-Curr Neurol Neurosci Rep-2009Beny RiliantoÎncă nu există evaluări
- Stroke BP 24 HrsDocument11 paginiStroke BP 24 HrsrodribeatsÎncă nu există evaluări
- Tadevosyan 2021Document26 paginiTadevosyan 2021W Antonio Rivera MartínezÎncă nu există evaluări
- Efficacy and Safety of Amlodipine Versus Captopril and Their Combination Inhypertensive Urgency A Randomized Controlled Trial 2329 9126 1000274Document7 paginiEfficacy and Safety of Amlodipine Versus Captopril and Their Combination Inhypertensive Urgency A Randomized Controlled Trial 2329 9126 1000274Laras OktavianiÎncă nu există evaluări
- Targeted Treatment of Severe Head Injury Based on Monitoring of Secondary InjuryDocument4 paginiTargeted Treatment of Severe Head Injury Based on Monitoring of Secondary InjuryAstari RahayuningtyasÎncă nu există evaluări
- Outcome Following Decompressive Craniectomy in Severe Head Injury - Rashid Hospital ExperienceDocument7 paginiOutcome Following Decompressive Craniectomy in Severe Head Injury - Rashid Hospital ExperienceSyafiq IshakÎncă nu există evaluări
- SSH en HTE. J Neuros 2012Document12 paginiSSH en HTE. J Neuros 2012Laura López Del Castillo LalydelcaÎncă nu există evaluări
- Traumatic Head InjuriesDocument50 paginiTraumatic Head InjuriesVasudha BuddyÎncă nu există evaluări
- Edema Cerebral UPTODATEDocument32 paginiEdema Cerebral UPTODATEChristian Andres Cruz PerezÎncă nu există evaluări
- Cerebral Herniation Syndromes and Intracranial HypertensionDe la EverandCerebral Herniation Syndromes and Intracranial HypertensionMatthew KoenigÎncă nu există evaluări
- Sudden Death: Advances in Diagnosis and TreatmentDe la EverandSudden Death: Advances in Diagnosis and TreatmentHaiyan ZhuÎncă nu există evaluări
- PsikososialDocument8 paginiPsikososialFatanahÎncă nu există evaluări
- Program PaliatifDocument10 paginiProgram PaliatifTheresia Avila KurniaÎncă nu există evaluări
- Status Gizi Ibu Saat Hamil, Berat Badan Lahir Bayi Dengan Stunting Pada BalitaDocument7 paginiStatus Gizi Ibu Saat Hamil, Berat Badan Lahir Bayi Dengan Stunting Pada BalitaDewa Ray Yunita SariÎncă nu există evaluări
- Jurnal Gizi Dan PanganDocument8 paginiJurnal Gizi Dan PanganUchiha Albert PardedeÎncă nu există evaluări
- Status Gizi Ibu Saat Hamil, Berat Badan Lahir Bayi Dengan Stunting Pada BalitaDocument7 paginiStatus Gizi Ibu Saat Hamil, Berat Badan Lahir Bayi Dengan Stunting Pada BalitaDewa Ray Yunita SariÎncă nu există evaluări
- Hasil Seleksi SNMPTN 2019 UnpadDocument41 paginiHasil Seleksi SNMPTN 2019 Unpadpkm pelindung hewanÎncă nu există evaluări
- 2520 4993 1 SMDocument8 pagini2520 4993 1 SMVeraÎncă nu există evaluări
- Disorders of Endocrine System: Prof. J. Hanáček, MD, PHDDocument66 paginiDisorders of Endocrine System: Prof. J. Hanáček, MD, PHDjerinthomasrajanÎncă nu există evaluări
- Lakip Yankes Tahun 2016Document1 paginăLakip Yankes Tahun 2016Theresia Avila KurniaÎncă nu există evaluări
- InfodatinDocument13 paginiInfodatinTheresia Avila KurniaÎncă nu există evaluări
- Principles of Anatomy and Physiology: The Endocrine SystemDocument84 paginiPrinciples of Anatomy and Physiology: The Endocrine SystemTheresia Avila KurniaÎncă nu există evaluări
- Who NMH NHD 14.5 EngDocument8 paginiWho NMH NHD 14.5 EngAsty PuthryyÎncă nu există evaluări
- Review: Factors Relating To Nurses' Caring Behaviors For Dying PatientsDocument13 paginiReview: Factors Relating To Nurses' Caring Behaviors For Dying PatientsFrederick BaldemoroÎncă nu există evaluări
- Rencana Anggaran 2016 PDFDocument27 paginiRencana Anggaran 2016 PDFLibriantyÎncă nu există evaluări
- 2520 4993 1 SMDocument8 pagini2520 4993 1 SMVeraÎncă nu există evaluări
- Journal of Career Assessment-2014-Chang PDFDocument14 paginiJournal of Career Assessment-2014-Chang PDFTheresia Avila KurniaÎncă nu există evaluări
- LiverpoolSedation ManagementDocument9 paginiLiverpoolSedation ManagementTheresia Avila KurniaÎncă nu există evaluări
- Guillain Barre SyndromeDocument2 paginiGuillain Barre SyndromeTheresia Avila KurniaÎncă nu există evaluări
- Guide To The Care of The Patient With PDFDocument41 paginiGuide To The Care of The Patient With PDFDaniel CainÎncă nu există evaluări
- Guillain Barre SyndromeDocument2 paginiGuillain Barre SyndromeTheresia Avila KurniaÎncă nu există evaluări
- Marketplace Provider Reimbursement ManualDocument270 paginiMarketplace Provider Reimbursement ManualTheresia Avila KurniaÎncă nu există evaluări
- 10 1016@j Resuscitation 2015 08 020Document6 pagini10 1016@j Resuscitation 2015 08 020Theresia Avila KurniaÎncă nu există evaluări
- Understanding Guillain-Barré Syndrome and Myasthenia GravisDocument31 paginiUnderstanding Guillain-Barré Syndrome and Myasthenia GravisTheresia Avila KurniaÎncă nu există evaluări
- Approach To The Infant or Child With Nausea and Vomiting - UpToDateDocument47 paginiApproach To The Infant or Child With Nausea and Vomiting - UpToDatemayteveronica1000Încă nu există evaluări
- PhysioEx Exercise 9 Activity 5Document3 paginiPhysioEx Exercise 9 Activity 5MARILYN MARIANA HERNANDEZ MENDOZAÎncă nu există evaluări
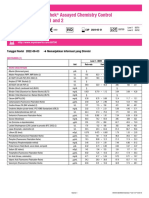
- Lyphochek Assayed Chemistry Control Levels 1 and 2: Tanggal Revisi 2022-06-03 Menunjukkan Informasi Yang DirevisiDocument2 paginiLyphochek Assayed Chemistry Control Levels 1 and 2: Tanggal Revisi 2022-06-03 Menunjukkan Informasi Yang DirevisiFahmiÎncă nu există evaluări
- Anatomy of The Left EyeDocument3 paginiAnatomy of The Left EyeJaessa FelicianoÎncă nu există evaluări
- Cambridge International General Certificate of Secondary EducationDocument16 paginiCambridge International General Certificate of Secondary EducationJeet JeetÎncă nu există evaluări
- Physical Exam of the Eye: Structures, Findings, DiagnosesDocument16 paginiPhysical Exam of the Eye: Structures, Findings, DiagnosesriveliÎncă nu există evaluări
- Surah Al An'aam (6:99) - Green Factory in PlantsDocument3 paginiSurah Al An'aam (6:99) - Green Factory in PlantsMuhammad Awais TahirÎncă nu există evaluări
- Imaging Modalities For Lung DiseasesDocument14 paginiImaging Modalities For Lung DiseasesYnaffit Alteza Untal100% (1)
- Feeding The Hemodinamically Unstable Patient A Critical Evolution of The EvidenceDocument9 paginiFeeding The Hemodinamically Unstable Patient A Critical Evolution of The EvidenceYanes NatanaelÎncă nu există evaluări
- Problems with Polyvagal TheoryDocument6 paginiProblems with Polyvagal TheoryCamilo IgnacioÎncă nu există evaluări
- Class X Biology Assignment Chapter 6 Life ProcessesDocument2 paginiClass X Biology Assignment Chapter 6 Life ProcessesVivek Nijhawan100% (1)
- Botany II PDFDocument7 paginiBotany II PDFMuhammad AmirÎncă nu există evaluări
- Macmillan Science Level 4 Pupil S Book Unit 1 PP 11 16Document6 paginiMacmillan Science Level 4 Pupil S Book Unit 1 PP 11 16reema2050reemaÎncă nu există evaluări
- Bipap A30 Specification / Part NumbersDocument2 paginiBipap A30 Specification / Part NumbersDejan ŽujovićÎncă nu există evaluări
- Jan 07 Old SNAB Unit 1 MSDocument10 paginiJan 07 Old SNAB Unit 1 MSCeleste FernandesÎncă nu există evaluări
- 10 Urinary BladderDocument32 pagini10 Urinary BladderMarera DomnicÎncă nu există evaluări
- A6. Karring T, Lang N, Löe H. The Role of Gingival Connective Tissue in Determining Epithelial Differentiation. J Perio Res 1975Document12 paginiA6. Karring T, Lang N, Löe H. The Role of Gingival Connective Tissue in Determining Epithelial Differentiation. J Perio Res 1975Daniel CubasÎncă nu există evaluări
- Company Most Recent Adposition (S) First Name Last Name Contact TypeDocument8 paginiCompany Most Recent Adposition (S) First Name Last Name Contact TypepaytencasÎncă nu există evaluări
- Photosynthesis WorksheetDocument3 paginiPhotosynthesis WorksheetByambazaya E100% (2)
- Somatic HybridizationDocument23 paginiSomatic HybridizationJan VivienelÎncă nu există evaluări
- Thesis Reza Salman Roghani PDFDocument76 paginiThesis Reza Salman Roghani PDFscoopyÎncă nu există evaluări
- Answer Guide For O Level Biology (5090/3) - Paper 3 Practical Test June 2001Document3 paginiAnswer Guide For O Level Biology (5090/3) - Paper 3 Practical Test June 2001MSHÎncă nu există evaluări
- Strain SprainDocument17 paginiStrain SprainPuterinugraha Wanca ApatyaÎncă nu există evaluări