S-ar putea să vă placă și
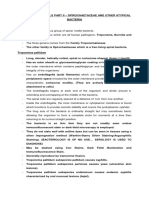
- Spirochetes and Atypical BacteriaDocument14 paginiSpirochetes and Atypical BacteriachippaiÎncă nu există evaluări
- Document 2Document1 paginăDocument 2chippaiÎncă nu există evaluări
- Streptococcus FinalDocument15 paginiStreptococcus FinalchippaiÎncă nu există evaluări
- Chippai 2Document1 paginăChippai 2chippaiÎncă nu există evaluări
- Vitek 2 Compact Brochure PDFDocument2 paginiVitek 2 Compact Brochure PDFchippaiÎncă nu există evaluări
- Para Report WordDocument3 paginiPara Report WordchippaiÎncă nu există evaluări
- Para Report WordDocument3 paginiPara Report WordchippaiÎncă nu există evaluări
- Francis Resume 2Document2 paginiFrancis Resume 2chippaiÎncă nu există evaluări
- Cc1 and 2 Comprehensive Reviewer (All Important)Document6 paginiCc1 and 2 Comprehensive Reviewer (All Important)chippaiÎncă nu există evaluări
- Document 2Document1 paginăDocument 2chippaiÎncă nu există evaluări
- QweqweqweDocument2 paginiQweqweqwechippaiÎncă nu există evaluări
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Cestode Parasites: Medical Parasitology, 2009 University of Palangkaraya Agus HaryonoDocument45 paginiCestode Parasites: Medical Parasitology, 2009 University of Palangkaraya Agus HaryonoMeylisa Gerson BayanÎncă nu există evaluări
- 11 16Document128 pagini11 16WoodsÎncă nu există evaluări
- Ascaris Suum PDFDocument6 paginiAscaris Suum PDFAdinda RahmaÎncă nu există evaluări
- Anatomy of The Uvea: Ruth Antolin, MD Doh Eye CenterDocument75 paginiAnatomy of The Uvea: Ruth Antolin, MD Doh Eye CenterRuth AntolinÎncă nu există evaluări
- Pigeon & Dove RescueDocument270 paginiPigeon & Dove RescuestormbrushÎncă nu există evaluări
- Annotated BibliographyDocument31 paginiAnnotated BibliographyLara MelissaÎncă nu există evaluări
- Lecture Notes - BIOS1170B (Body Systems - (Structure and Function) ) (Sydney)Document86 paginiLecture Notes - BIOS1170B (Body Systems - (Structure and Function) ) (Sydney)SK AuÎncă nu există evaluări
- Diarrhea RoleplayDocument5 paginiDiarrhea Roleplayidabagus putuwidanaÎncă nu există evaluări
- Cheat Sheet 2Document2 paginiCheat Sheet 2oushaÎncă nu există evaluări
- Import Requirements (NEW)Document15 paginiImport Requirements (NEW)Thiago NunesÎncă nu există evaluări
- A - Mallard DuckDocument24 paginiA - Mallard DuckcmembreveÎncă nu există evaluări
- What Is Tetralogy of FallotDocument2 paginiWhat Is Tetralogy of FallotJamaica Cruz San Pedro100% (1)
- Tympanic MembraneDocument13 paginiTympanic MembraneJerry NgÎncă nu există evaluări
- CBSE Class 7 English - Comprehension PassageDocument7 paginiCBSE Class 7 English - Comprehension PassagemotherhoodÎncă nu există evaluări
- Ocw Humanos y Otros AnimalesDocument4 paginiOcw Humanos y Otros Animalesmiguel6789Încă nu există evaluări
- Đề 4. Đề Thi Thử TN THPT Môn Tiếng Anh Theo Cấu Trúc Đề Minh Họa 2021 - Cô Oanh - Có Lời GiảiDocument15 paginiĐề 4. Đề Thi Thử TN THPT Môn Tiếng Anh Theo Cấu Trúc Đề Minh Họa 2021 - Cô Oanh - Có Lời GiảiBình Bùi thanhÎncă nu există evaluări
- BIOLOGY RevisionNotes SaveMyExamsDocument7 paginiBIOLOGY RevisionNotes SaveMyExamsAli AshrafÎncă nu există evaluări
- Cardiac MonitorDocument3 paginiCardiac MonitorShameera M. KamlianÎncă nu există evaluări
- Refinements in The Care and Use of Animals in Toxicology Studies - Regulation, Validation and ProgressDocument8 paginiRefinements in The Care and Use of Animals in Toxicology Studies - Regulation, Validation and Progressgabriela_mariangela5929Încă nu există evaluări
- Breast Care in BreastfeedingDocument11 paginiBreast Care in BreastfeedingBella Cy LopezÎncă nu există evaluări
- Vaccines CHNDocument2 paginiVaccines CHNLyra LorcaÎncă nu există evaluări
- Vol 28 No 2 Dec 2004 - 1 Topic Covered by Subba RaoDocument80 paginiVol 28 No 2 Dec 2004 - 1 Topic Covered by Subba Raoabtester0% (1)
- 144 Diagnosa FKTPDocument5 pagini144 Diagnosa FKTPpuskesmas100% (1)
- ЧАРАКА-САМХИТА СУТРАСТХАНАDocument218 paginiЧАРАКА-САМХИТА СУТРАСТХАНАTremayne HansenÎncă nu există evaluări
- Reproduction SystemDocument38 paginiReproduction SystemNurfatin AdilaÎncă nu există evaluări
- Cs Breast EngorgementDocument14 paginiCs Breast Engorgementamit85% (13)
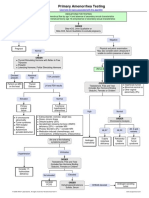
- Primary Amenorrhea Testing AlgorithmDocument1 paginăPrimary Amenorrhea Testing AlgorithmGabriella AguirreÎncă nu există evaluări
- Terror of Athas 3.5EDocument199 paginiTerror of Athas 3.5EÉricGaudet100% (2)
- Ccypi 3.0Document76 paginiCcypi 3.0GirishÎncă nu există evaluări
- Tutorial Dr. SaugiDocument33 paginiTutorial Dr. SaugifemmytaniaÎncă nu există evaluări