S-ar putea să vă placă și
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (399)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Psychological Assessment ReviewerDocument9 paginiPsychological Assessment Reviewerpatquianzon100% (1)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (73)
- Framingham Risk Score SaDocument8 paginiFramingham Risk Score Saapi-301624030Încă nu există evaluări
- My Sister's KeeperDocument3 paginiMy Sister's Keeperbetsyk1Încă nu există evaluări
- Jodi Halpern - From Detached Concern To EmpathyDocument188 paginiJodi Halpern - From Detached Concern To Empathycobby174100% (1)
- Adsorption PresentationDocument23 paginiAdsorption Presentationarun231187100% (1)
- How to prepare your Asil for fightingDocument16 paginiHow to prepare your Asil for fightingcinna01Încă nu există evaluări
- Carbohydrates 131204014552 Phpapp02 PDFDocument27 paginiCarbohydrates 131204014552 Phpapp02 PDFTweenie Dalumpines100% (4)
- Uttar Pradesh Empanelment List for Minilap 2018-19Document19 paginiUttar Pradesh Empanelment List for Minilap 2018-19Vijay KumarÎncă nu există evaluări
- A Devoted SonDocument1 paginăA Devoted SonAnkur MaheshwariÎncă nu există evaluări
- ChromatographyDocument31 paginiChromatographyarun231187Încă nu există evaluări
- Farm NoteDocument3 paginiFarm NoteSreya Sanil50% (2)
- Advances in Psychological and Social Support After DisastersDocument149 paginiAdvances in Psychological and Social Support After DisastersjprewittdiazÎncă nu există evaluări
- PhysiologicalrolesofmineralsDocument46 paginiPhysiologicalrolesofmineralsarun231187Încă nu există evaluări
- XRDDocument27 paginiXRDHardik PrajapatiÎncă nu există evaluări
- Composition and FunctionsDocument13 paginiComposition and Functionsarun231187Încă nu există evaluări
- Paperchromatographybharmsud 151012115319 Lva1 App6891 PDFDocument34 paginiPaperchromatographybharmsud 151012115319 Lva1 App6891 PDFarun231187Încă nu există evaluări
- PUB210 HemeAtlas SampleDocument6 paginiPUB210 HemeAtlas Samplearun231187Încă nu există evaluări
- Vogel ExtractDocument17 paginiVogel Extractarun231187Încă nu există evaluări
- International University of Africa Faculty of Pharmacy Medicinal Chemistry MCHM 311 Siddieg Omer Elsiddieg, M. SC, B. SC (Honors)Document47 paginiInternational University of Africa Faculty of Pharmacy Medicinal Chemistry MCHM 311 Siddieg Omer Elsiddieg, M. SC, B. SC (Honors)arun231187Încă nu există evaluări
- Conductometry Titrations PDFDocument4 paginiConductometry Titrations PDFkomalseemi97Încă nu există evaluări
- Specific Immune System: T - LymphocytesDocument18 paginiSpecific Immune System: T - Lymphocytesarun231187Încă nu există evaluări
- Ureacycle ConversionDocument31 paginiUreacycle Conversionarun231187Încă nu există evaluări
- Effective Communication Between Physician and Pharmacist: Dr. G Praveen KumarDocument50 paginiEffective Communication Between Physician and Pharmacist: Dr. G Praveen Kumararun231187Încă nu există evaluări
- TwocomponentsystemDocument28 paginiTwocomponentsystemarun231187Încă nu există evaluări
- High Energy Compouds: Anjali.H.S BCH.10.05.10Document66 paginiHigh Energy Compouds: Anjali.H.S BCH.10.05.10arun231187Încă nu există evaluări
- Introduction to Biochemistry FundamentalsDocument34 paginiIntroduction to Biochemistry Fundamentalsarun231187Încă nu există evaluări
- CARBOHYDRATESDocument38 paginiCARBOHYDRATESgulrukh100% (3)
- Calibracion MicropipetasDocument4 paginiCalibracion MicropipetasAnonymous 58LGc3Încă nu există evaluări
- Carpalbonefractures 150330093618 Conversion Gate01Document136 paginiCarpalbonefractures 150330093618 Conversion Gate01arun231187Încă nu există evaluări
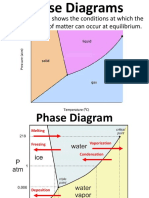
- A Phase Diagram Shows The Conditions at Which The Distinct Phases of Matter Can Occur at EquilibriumDocument9 paginiA Phase Diagram Shows The Conditions at Which The Distinct Phases of Matter Can Occur at Equilibriumarun231187Încă nu există evaluări
- ThephaseruleDocument48 paginiThephaserulearun231187Încă nu există evaluări
- 4 ImportanceofbiochemistryDocument18 pagini4 Importanceofbiochemistryarun231187Încă nu există evaluări
- Pipette CalibrationDocument79 paginiPipette Calibrationarun231187Încă nu există evaluări
- StalagmometerDocument4 paginiStalagmometerRamesh KumarÎncă nu există evaluări
- Nutrition 1101-Lecture 21Document21 paginiNutrition 1101-Lecture 21arun231187Încă nu există evaluări
- Pipette CalibrationDocument4 paginiPipette CalibrationbalajivangaruÎncă nu există evaluări
- Titrasi PresipitasiDocument85 paginiTitrasi PresipitasiayukiwaÎncă nu există evaluări
- 4 ImportanceofbiochemistryDocument18 pagini4 Importanceofbiochemistryarun231187Încă nu există evaluări
- Qualitative Carbohydrate Tests GuideDocument52 paginiQualitative Carbohydrate Tests Guidearun231187Încă nu există evaluări
- Cutera Laser Genesis Patient BrochureDocument6 paginiCutera Laser Genesis Patient BrochureRogier van der HeideÎncă nu există evaluări
- Continuous Passive Motion (CPM) : Theory and Principles of Clinical ApplicationDocument10 paginiContinuous Passive Motion (CPM) : Theory and Principles of Clinical ApplicationlaurentiaÎncă nu există evaluări
- Detyre Kursi: Lenda:AnglishtDocument11 paginiDetyre Kursi: Lenda:AnglishtFjorelo FeroÎncă nu există evaluări
- EORTC QLQ-C30 Into Indonesian VersionDocument11 paginiEORTC QLQ-C30 Into Indonesian VersionHendryÎncă nu există evaluări
- Narcotic Drugs: Opium Herion Codeine Tramadol MorphineDocument9 paginiNarcotic Drugs: Opium Herion Codeine Tramadol MorphineSyed renobaÎncă nu există evaluări
- Masters in Medical Science - MMSCDocument12 paginiMasters in Medical Science - MMSCtexilaamericanÎncă nu există evaluări
- Medical Council of Inida Declaration Form 2010-2011for FacultyDocument9 paginiMedical Council of Inida Declaration Form 2010-2011for FacultydrtpkÎncă nu există evaluări
- Types of Casts and Their IndicationsDocument3 paginiTypes of Casts and Their IndicationsPhylum ChordataÎncă nu există evaluări
- 53 Vol. 6 Issue 7 IJPSR 2015 RA 4953Document9 pagini53 Vol. 6 Issue 7 IJPSR 2015 RA 4953Dina AyupnÎncă nu există evaluări
- 0100 Sigmazam ReducerDocument2 pagini0100 Sigmazam ReducerAhmed SaadÎncă nu există evaluări
- 01 M039 43754Document16 pagini01 M039 43754DrDeepak PawarÎncă nu există evaluări
- Partners Case CCMNDocument4 paginiPartners Case CCMNapi-314349758Încă nu există evaluări
- It PDFDocument385 paginiIt PDFCosmina UngurÎncă nu există evaluări
- Replacing ESR with Plasma ViscosityDocument6 paginiReplacing ESR with Plasma ViscosityRyan ChenÎncă nu există evaluări
- Aos 94 10Document11 paginiAos 94 10Andi Tiara S. AdamÎncă nu există evaluări
- Isolating Staphylococcus SPDocument4 paginiIsolating Staphylococcus SPHani HairullaÎncă nu există evaluări
- Study The Herbalism of Thyme LeavesDocument7 paginiStudy The Herbalism of Thyme Leavespronto4meÎncă nu există evaluări
- Chapter1 Intro of Biomedical Signal ProcessingDocument50 paginiChapter1 Intro of Biomedical Signal ProcessingShafayet Uddin100% (3)
- Micro and Nanotechnologies in Tissue Engineering of Heart ValveDocument15 paginiMicro and Nanotechnologies in Tissue Engineering of Heart ValveMD Anwarul HasanÎncă nu există evaluări
- A Review On Netra Tarpana - An Ayurveda Method of Eye Care: January 2021Document10 paginiA Review On Netra Tarpana - An Ayurveda Method of Eye Care: January 2021Lepaksha GowdaÎncă nu există evaluări
- Footnote To YouthDocument6 paginiFootnote To YouthVanityHughÎncă nu există evaluări