S-ar putea să vă placă și
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (399)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (890)
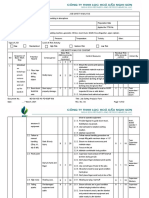
- JOB SAFETY ANALYSISDocument21 paginiJOB SAFETY ANALYSISThái Đạo Phạm Lê100% (1)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Read - Silverdale Rape LawsuitDocument16 paginiRead - Silverdale Rape LawsuitDan LehrÎncă nu există evaluări
- Apology Language Profile For Adults - The 5 Love Languages®Document3 paginiApology Language Profile For Adults - The 5 Love Languages®Dadar JagungÎncă nu există evaluări
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Ground HandlingDocument46 paginiGround HandlingIshwar ThapaÎncă nu există evaluări
- Hulda Clark - ZapperDocument113 paginiHulda Clark - ZapperCarlosÎncă nu există evaluări
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (73)
- How Emotion and the Human Brain Are Deeply IntertwinedDocument6 paginiHow Emotion and the Human Brain Are Deeply IntertwinedBruno XavierÎncă nu există evaluări
- Construction Safety HandbookDocument133 paginiConstruction Safety HandbookAngelica Valle RosaÎncă nu există evaluări
- Birth InjuriesDocument102 paginiBirth InjuriesmazlinamaidinÎncă nu există evaluări
- Crash CartDocument2 paginiCrash CartMenGuitarÎncă nu există evaluări
- ?actors Hidden Whore by ThexwhysDocument956 pagini?actors Hidden Whore by ThexwhysRed Jem100% (1)
- Foundations of Piano TechniqueDocument1 paginăFoundations of Piano TechniqueLukeÎncă nu există evaluări
- EFSA Journal - 2009.1413 (05.04.2021)Document21 paginiEFSA Journal - 2009.1413 (05.04.2021)Khaled BenzartiÎncă nu există evaluări
- Transvaginal scan findings and treatment planDocument4 paginiTransvaginal scan findings and treatment planJudy Ann CristeÎncă nu există evaluări
- Drug Study TranexamicDocument3 paginiDrug Study Tranexamicalpha mayagaÎncă nu există evaluări
- Mansion Brainstorming and Paraphrasing - Student SlideDocument35 paginiMansion Brainstorming and Paraphrasing - Student SlideVũ Nguyễn TuấnÎncă nu există evaluări
- Es 26 3 212Document11 paginiEs 26 3 212kang soon cheolÎncă nu există evaluări
- Effects of Rambutan Seeds To Blood GlucoseDocument4 paginiEffects of Rambutan Seeds To Blood GlucoseMonique Puspos San Lorenzo100% (1)
- Mediserve QLD Nurse Reg (Print)Document11 paginiMediserve QLD Nurse Reg (Print)Alex PiecesÎncă nu există evaluări
- Organizational Analysis of Sultan Kudarat Doctor's Hospital Nursing DepartmentDocument8 paginiOrganizational Analysis of Sultan Kudarat Doctor's Hospital Nursing DepartmentAnni BarbaÎncă nu există evaluări
- Diagnostic Test Battery For Different Age GroupsDocument14 paginiDiagnostic Test Battery For Different Age GroupsDhana KrishnaÎncă nu există evaluări
- Detailed Notification CRP PO XIIIDocument48 paginiDetailed Notification CRP PO XIIIGanesh ShindeÎncă nu există evaluări
- Personal Development Plan (PDP) Assignment: Your Plan Should Have The Following ComponentsDocument4 paginiPersonal Development Plan (PDP) Assignment: Your Plan Should Have The Following Componentstomar_muditÎncă nu există evaluări
- Examination & Diagnosis of Edentulous Patients: Presented By: Dr. Jehan Dordi 1 Yr. MdsDocument159 paginiExamination & Diagnosis of Edentulous Patients: Presented By: Dr. Jehan Dordi 1 Yr. MdsAkanksha MahajanÎncă nu există evaluări
- Process Analysis EssayDocument9 paginiProcess Analysis Essayapi-534788383Încă nu există evaluări
- PDF Anemia Concept Map0000Document1 paginăPDF Anemia Concept Map0000alvianmerzaradiputraÎncă nu există evaluări
- Powerpoint Presentation PathoDocument6 paginiPowerpoint Presentation Pathoapi-719781614Încă nu există evaluări
- Funda Rle Retdem ProceduresDocument9 paginiFunda Rle Retdem Proceduresaceh lorttÎncă nu există evaluări
- Psychoeducation For Severe Mental Illnesses Theory and Practice, Final Seminar PrintDocument22 paginiPsychoeducation For Severe Mental Illnesses Theory and Practice, Final Seminar PrintAnnPSWÎncă nu există evaluări
- Puerto Rico Building Codes GuideDocument3 paginiPuerto Rico Building Codes GuideTommyCasillas-GerenaÎncă nu există evaluări
- Report On Deworming: Rosario District Mayor Calixto D. Enriquez Elementary SchoolDocument1 paginăReport On Deworming: Rosario District Mayor Calixto D. Enriquez Elementary SchoolJoonEdFavilaGayagoyÎncă nu există evaluări