S-ar putea să vă placă și
- Electrocardiograma Neyssa KimeeDocument15 paginiElectrocardiograma Neyssa KimeeNEYSSA KIMEE SAINT VILÎncă nu există evaluări
- Lesson 4Document3 paginiLesson 4NER CARLO SANTOSÎncă nu există evaluări
- Advances in CT FinalDocument61 paginiAdvances in CT Finalranandkumarmech_3205Încă nu există evaluări
- Hong 2019Document5 paginiHong 2019anggita ningratÎncă nu există evaluări
- Fact or Artifact in Two-Dimensional EchocardiographyDocument27 paginiFact or Artifact in Two-Dimensional EchocardiographyAndreza Patricia Marinho de Souza MartinsÎncă nu există evaluări
- Pollak Et Al 2012 Multimodality Imaging of Lower Extremity Peripheral Arterial DiseaseDocument11 paginiPollak Et Al 2012 Multimodality Imaging of Lower Extremity Peripheral Arterial DiseasePatricia Peñaflor GrimaldoÎncă nu există evaluări
- Aortic AneurysmDocument17 paginiAortic AneurysmTeguh Imana NugrahaÎncă nu există evaluări
- Jead 024Document21 paginiJead 024wassim wassimÎncă nu există evaluări
- Handouts 1Document12 paginiHandouts 1banana_rockÎncă nu există evaluări
- Unit 1 Basics of Echocardiography and Cardiac DopplerDocument29 paginiUnit 1 Basics of Echocardiography and Cardiac DopplerJack TomarÎncă nu există evaluări
- J Nucl Med-1994-DePuey-699-702Document5 paginiJ Nucl Med-1994-DePuey-699-702alinaÎncă nu există evaluări
- Akkaya 2018Document7 paginiAkkaya 2018Carolina ValenzuelaÎncă nu există evaluări
- Clinical Applications of Ultrasonography in Neurocritically Ill PatientsDocument8 paginiClinical Applications of Ultrasonography in Neurocritically Ill PatientsEstefania RomanÎncă nu există evaluări
- New Advances in Wrist ArthrosDocument13 paginiNew Advances in Wrist ArthrosDiego Maté MartínÎncă nu există evaluări
- Mehran1999 220903 094007Document9 paginiMehran1999 220903 094007Nasru llahÎncă nu există evaluări
- CT ANGIOGRAPHY - DETAILED IMAGES OF BLOOD VESSELSDocument1 paginăCT ANGIOGRAPHY - DETAILED IMAGES OF BLOOD VESSELSsreejithÎncă nu există evaluări
- Fvets 09 819627Document12 paginiFvets 09 819627Ana AldazÎncă nu există evaluări
- 227 Full PDFDocument3 pagini227 Full PDFanon_629352389Încă nu există evaluări
- Use of Intracoronary ImagingDocument11 paginiUse of Intracoronary ImagingPhyoNyeinChanÎncă nu există evaluări
- SMI - A New Technique For The Analysis of The Microvascular Tree in Reactive and Suspected Malignant Lymphadenopathy in Advanced Stages of Malignant MelanomaDocument6 paginiSMI - A New Technique For The Analysis of The Microvascular Tree in Reactive and Suspected Malignant Lymphadenopathy in Advanced Stages of Malignant MelanomaAlexa1202Încă nu există evaluări
- Diagnosis of Atherosclerosis by Imaging. - AJM.2008Document11 paginiDiagnosis of Atherosclerosis by Imaging. - AJM.2008Carlos MurilloÎncă nu există evaluări
- Jurnal ReadingDocument7 paginiJurnal ReadingHanif UlinÎncă nu există evaluări
- Ajnr A6171 FullDocument9 paginiAjnr A6171 FullDuraidÎncă nu există evaluări
- Acute Traumatic Knee RadiographsDocument10 paginiAcute Traumatic Knee RadiographsPrashant GuptaÎncă nu există evaluări
- Proyecciones EuroInterventionDocument2 paginiProyecciones EuroInterventionLuis Enrique Giraldo PenicheÎncă nu există evaluări
- Coronary CTA ReviewDocument4 paginiCoronary CTA ReviewRedhwan Abdullah qaid AlshubiÎncă nu există evaluări
- 2020 EuroInterv - OCT Rota Vs IVUS RotaDocument9 pagini2020 EuroInterv - OCT Rota Vs IVUS RotaTeng Hsin-IÎncă nu există evaluări
- Chapter 01 - Principles of Echocardiography - 1Document12 paginiChapter 01 - Principles of Echocardiography - 1maca_mike5723Încă nu există evaluări
- PJR 85 41637Document20 paginiPJR 85 41637Rakesh JhaÎncă nu există evaluări
- WJR 6 355Document12 paginiWJR 6 355Victor ChiabaiÎncă nu există evaluări
- Hitachi-Aloka Arietta 70 BrochureDocument15 paginiHitachi-Aloka Arietta 70 BrochureDANIA BWIDANIÎncă nu există evaluări
- Ultrasonografia em EquinosDocument8 paginiUltrasonografia em EquinosIngrid MachadoÎncă nu există evaluări
- Brain AVM Embolization with Onyx: Initial Experience with a New Liquid Embolic AgentDocument6 paginiBrain AVM Embolization with Onyx: Initial Experience with a New Liquid Embolic AgentCut FadmalaÎncă nu există evaluări
- Scanning Systems, Ultrasonic, Cardiac Intravascular: Scope of This Product ComparisonDocument75 paginiScanning Systems, Ultrasonic, Cardiac Intravascular: Scope of This Product Comparisonkevin. mitnickÎncă nu există evaluări
- Arrhythmia Recognition and Classification Using Combined Parametric and Visual Pattern Features of ECG MorphologyDocument15 paginiArrhythmia Recognition and Classification Using Combined Parametric and Visual Pattern Features of ECG MorphologyAhmed AlrefaiÎncă nu există evaluări
- Doppler Transcreaneal y Ecografía Del Nervio ÓpticoDocument15 paginiDoppler Transcreaneal y Ecografía Del Nervio ÓpticoBenjamínGalvanÎncă nu există evaluări
- Diagnoses SDocument25 paginiDiagnoses STudor DumitrascuÎncă nu există evaluări
- Cerebral AngiographyDocument3 paginiCerebral AngiographyBiway RegalaÎncă nu există evaluări
- Atlas c1Document5 paginiAtlas c1davorribicicÎncă nu există evaluări
- 200468-001 - ANTERION - ANTERION-Image-Book - EN PDFDocument13 pagini200468-001 - ANTERION - ANTERION-Image-Book - EN PDFJulio AtencioÎncă nu există evaluări
- Echocardiographic Assessment of Myocardial Strain: John Gorcsan III, MD, Hidekazu Tanaka, MDDocument13 paginiEchocardiographic Assessment of Myocardial Strain: John Gorcsan III, MD, Hidekazu Tanaka, MDJorge Luis Jara ValderramaÎncă nu există evaluări
- Assessment of Left Ventricular Myocardial Diseases With Cardiac Computed TomographyDocument19 paginiAssessment of Left Ventricular Myocardial Diseases With Cardiac Computed Tomographysyifa auliaÎncă nu există evaluări
- Positioning Ppt. 1Document53 paginiPositioning Ppt. 1Echo Gumolda WandaganÎncă nu există evaluări
- Canon Vantage Elan Brochure enDocument13 paginiCanon Vantage Elan Brochure enrhodes mwaitaÎncă nu există evaluări
- Vascular Imaging EquipmentsDocument50 paginiVascular Imaging EquipmentsRohit nikamÎncă nu există evaluări
- Coronary Anatomy With Multidetector Computed Tomography AngiographyDocument7 paginiCoronary Anatomy With Multidetector Computed Tomography AngiographyAndré luisÎncă nu există evaluări
- Week 7 NeckDocument29 paginiWeek 7 NeckAbbas OmerÎncă nu există evaluări
- Claus 2015Document17 paginiClaus 2015Dr. Muha. Hasan Mahbub-Ur-RahmanÎncă nu există evaluări
- 2019-TMI-Cardiac Phase Detection in EchocardiogramsDocument12 pagini2019-TMI-Cardiac Phase Detection in EchocardiogramsZhenyu BuÎncă nu există evaluări
- Angio IRMDocument8 paginiAngio IRMAndreea MunteanuÎncă nu există evaluări
- Mri 10Document16 paginiMri 10Hatem DheerÎncă nu există evaluări
- Euroscore IiDocument5 paginiEuroscore IiYadira SantosÎncă nu există evaluări
- Unenhanced MR Angiography: Martin Backens and Bernd SchmitzDocument20 paginiUnenhanced MR Angiography: Martin Backens and Bernd SchmitzEka Setyorini .A.Încă nu există evaluări
- Biomedical Instruments Classification GuideDocument53 paginiBiomedical Instruments Classification GuideSujith SurendranÎncă nu există evaluări
- Masas Cardiacas Parte 1 PMC 2015Document13 paginiMasas Cardiacas Parte 1 PMC 2015Diego Andrés Mejía VascoÎncă nu există evaluări
- Role of Echocardiographic Imaging in PercutaneousDocument10 paginiRole of Echocardiographic Imaging in PercutaneousAnonymous 9wHscMÎncă nu există evaluări
- The Role of AI in The Echocardiogrphy Worklow 1699588143Document8 paginiThe Role of AI in The Echocardiogrphy Worklow 1699588143giovannimacÎncă nu există evaluări
- Decoding Cardiac Electrophysiology: Understanding the Techniques and Defining the JargonDe la EverandDecoding Cardiac Electrophysiology: Understanding the Techniques and Defining the JargonAfzal SohaibÎncă nu există evaluări
- Atlas of Coronary Intravascular Optical Coherence TomographyDe la EverandAtlas of Coronary Intravascular Optical Coherence TomographyÎncă nu există evaluări
- Atlas of CT Angiography: Normal and Pathologic FindingsDe la EverandAtlas of CT Angiography: Normal and Pathologic FindingsÎncă nu există evaluări
- Zoom LInkDocument2 paginiZoom LInkMitulsinh M RavaljiÎncă nu există evaluări
- Instructions To Student 'S: Student Can Use Cam Scanner App For Scanning The Paper)Document1 paginăInstructions To Student 'S: Student Can Use Cam Scanner App For Scanning The Paper)Mitulsinh M RavaljiÎncă nu există evaluări
- Revision TTDocument2 paginiRevision TTMitulsinh M RavaljiÎncă nu există evaluări
- Save Environment Poster TipsDocument1 paginăSave Environment Poster TipsMitulsinh M RavaljiÎncă nu există evaluări
- Rebirth of India PDFDocument15 paginiRebirth of India PDFsrivenraman33% (3)
- Annual Exam Time TableDocument1 paginăAnnual Exam Time TableMitulsinh M RavaljiÎncă nu există evaluări
- Types of Rocks - Igneous, Sedimentary, MetamorphicDocument1 paginăTypes of Rocks - Igneous, Sedimentary, MetamorphicMitulsinh M RavaljiÎncă nu există evaluări
- UAE's 50 Years of Unity: The Nation's Iconic LogoDocument1 paginăUAE's 50 Years of Unity: The Nation's Iconic LogoMitulsinh M RavaljiÎncă nu există evaluări
- Nomination User Manual enDocument31 paginiNomination User Manual enMitulsinh M RavaljiÎncă nu există evaluări
- Word Problems - Division Word Problems SolvedDocument2 paginiWord Problems - Division Word Problems SolvedMitulsinh M RavaljiÎncă nu există evaluări
- Home Work: Science: Hindi: SSTDocument1 paginăHome Work: Science: Hindi: SSTMitulsinh M RavaljiÎncă nu există evaluări
- Save Our EnviromentDocument1 paginăSave Our EnviromentMitulsinh M RavaljiÎncă nu există evaluări
- Half Yearly Portions - Grade 6Document4 paginiHalf Yearly Portions - Grade 6Mitulsinh M RavaljiÎncă nu există evaluări
- Writing Radiology Reports in ChiropracticDocument6 paginiWriting Radiology Reports in ChiropracticRohit SagarÎncă nu există evaluări
- Shuchita Ravalji - G5 WS 1 Food and HealthDocument4 paginiShuchita Ravalji - G5 WS 1 Food and HealthMitulsinh M RavaljiÎncă nu există evaluări
- FAQs - May'20Document7 paginiFAQs - May'20Mitulsinh M RavaljiÎncă nu există evaluări
- Lagangito Ane RivajoDocument44 paginiLagangito Ane RivajoMitulsinh M RavaljiÎncă nu există evaluări
- CME On Renal Colic Pain and Beyond Pain!Document1 paginăCME On Renal Colic Pain and Beyond Pain!Mitulsinh M RavaljiÎncă nu există evaluări
- Ifgl Refractories: Executive SummaryDocument14 paginiIfgl Refractories: Executive SummaryMitulsinh M RavaljiÎncă nu există evaluări
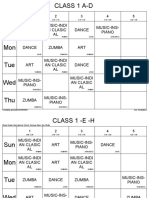
- ART Music-Indi An Clasic AL Music-Ins-Piano Dance: Global Indian International School, Baniyas East, Abu DhabiDocument8 paginiART Music-Indi An Clasic AL Music-Ins-Piano Dance: Global Indian International School, Baniyas East, Abu DhabiMitulsinh M RavaljiÎncă nu există evaluări
- Half Yearly Portions - Grade 6Document4 paginiHalf Yearly Portions - Grade 6Mitulsinh M RavaljiÎncă nu există evaluări
- New Timetable IiibDocument1 paginăNew Timetable IiibMitulsinh M RavaljiÎncă nu există evaluări
- Final School CalendarDocument19 paginiFinal School CalendarMitulsinh M RavaljiÎncă nu există evaluări
- SEHA - Employee HandbookDocument54 paginiSEHA - Employee Handbookasimasim123100% (1)
- Math NotesDocument25 paginiMath NotesMitulsinh M RavaljiÎncă nu există evaluări
- Ambit-Chemicals POSITIVE A Never Before World-22-04-2020 08-29-53Document65 paginiAmbit-Chemicals POSITIVE A Never Before World-22-04-2020 08-29-53RaviTejaÎncă nu există evaluări
- Numbers Up To 200: 1. Fill in The Missing Numbers in The Grid. Complete Each RowDocument6 paginiNumbers Up To 200: 1. Fill in The Missing Numbers in The Grid. Complete Each RowMitulsinh M RavaljiÎncă nu există evaluări
- Ganpati Path in Gujarati PDFDocument1 paginăGanpati Path in Gujarati PDFMitulsinh M Ravalji0% (1)
- Regulation for Radiation Dose Limits and OptimisationDocument11 paginiRegulation for Radiation Dose Limits and OptimisationMitulsinh M RavaljiÎncă nu există evaluări
- Ambit-Chemicals POSITIVE A Never Before World-22-04-2020 08-29-53Document65 paginiAmbit-Chemicals POSITIVE A Never Before World-22-04-2020 08-29-53RaviTejaÎncă nu există evaluări
- LBADocument3 paginiLBARajeev AgurÎncă nu există evaluări
- ĒTHRANE (Enflurane, USP) : Liquid For Inhalation R Only DescriptionDocument9 paginiĒTHRANE (Enflurane, USP) : Liquid For Inhalation R Only Descriptiondevi arianiÎncă nu există evaluări
- Niacin Chemical Forms, Bioavailability, and Health EffectsDocument10 paginiNiacin Chemical Forms, Bioavailability, and Health EffectsNutri_InfoÎncă nu există evaluări
- Jurnal PDPH Anest RisaDocument15 paginiJurnal PDPH Anest Risaadit rifqiÎncă nu există evaluări
- S3 Guideline Androgenetic Alopecia Update2017Document101 paginiS3 Guideline Androgenetic Alopecia Update2017redhacuÎncă nu există evaluări
- Chapter 13 Cleft Palate PDFDocument21 paginiChapter 13 Cleft Palate PDFmitasarisukadanaÎncă nu există evaluări
- 2.radiation Biology Q & ADocument7 pagini2.radiation Biology Q & AdrpnnreddyÎncă nu există evaluări
- Chronic Benign Paroxysmal Positional Vertigo (BPPVDocument2 paginiChronic Benign Paroxysmal Positional Vertigo (BPPVicarosalernoÎncă nu există evaluări
- Pediatric Anesthesia BasicsDocument24 paginiPediatric Anesthesia Basicsvani_kalai005Încă nu există evaluări
- MH CBIS ManualDocument79 paginiMH CBIS ManualAnonymous Ax12P2srÎncă nu există evaluări
- ROP Operational Guidelines FINAL PDFDocument58 paginiROP Operational Guidelines FINAL PDFRajan ShuklaÎncă nu există evaluări
- Lower Extremity DisordersDocument14 paginiLower Extremity DisordersJameson87Încă nu există evaluări
- 14 Cancer Symptoms Women Ignore - 3Document1 pagină14 Cancer Symptoms Women Ignore - 3Meidi RaniÎncă nu există evaluări
- PaxilDocument5 paginiPaxilSandro AlcobaçaÎncă nu există evaluări
- Nick Franks - Chapter 14 Instruments and Codes FN v2 - Rev 3 For Radionic Journal 17.4.15Document19 paginiNick Franks - Chapter 14 Instruments and Codes FN v2 - Rev 3 For Radionic Journal 17.4.15evandrojsilvaÎncă nu există evaluări
- PerdevDocument33 paginiPerdevBatchie Bugs StuartÎncă nu există evaluări
- Tots SlidesDocument179 paginiTots Slidesamarneh1969Încă nu există evaluări
- Suffolk 2023 Directory Care HomesDocument80 paginiSuffolk 2023 Directory Care HomesChey1242Încă nu există evaluări
- From A Pathologist's DeskDocument33 paginiFrom A Pathologist's DeskDr Suvarna NalapatÎncă nu există evaluări
- Case Report RADocument66 paginiCase Report RAAdibah TajuddinÎncă nu există evaluări
- DR - Syafrizal NST, SP - PDDocument69 paginiDR - Syafrizal NST, SP - PDDenis Harli SiregarÎncă nu există evaluări
- Labor and Delivery QuizDocument7 paginiLabor and Delivery QuizAmy50% (2)
- Jurnal GLIKOSIDA ALKOHOL White Willow Bark (Salix Alba)Document12 paginiJurnal GLIKOSIDA ALKOHOL White Willow Bark (Salix Alba)Akhmad NgafifÎncă nu există evaluări
- ICU patient transfer guidelineDocument8 paginiICU patient transfer guidelineInnas DoankÎncă nu există evaluări
- Literature Review: Periodontal AnatomyDocument68 paginiLiterature Review: Periodontal AnatomyRoshna NarayanÎncă nu există evaluări
- Hallucinations and Hearing VoicesDocument5 paginiHallucinations and Hearing VoicesdevÎncă nu există evaluări
- Autistic Adult Perspectives On Occupational Therapy For Autistic Children and YouthDocument8 paginiAutistic Adult Perspectives On Occupational Therapy For Autistic Children and YouthNataliaÎncă nu există evaluări
- The Empirical Study of PsychoanalysisDocument22 paginiThe Empirical Study of PsychoanalysisAriel PollakÎncă nu există evaluări
- RRLDocument3 paginiRRLKevin M. VillacorteÎncă nu există evaluări
- 403-1 VersamedLM IventDocument9 pagini403-1 VersamedLM IventCARLOS2285Încă nu există evaluări