S-ar putea să vă placă și
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
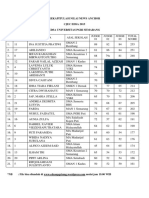
- NO NO Undian Nama Asal Sekolah Judge 01 Judge 02 Judge 03 Total ScoreDocument6 paginiNO NO Undian Nama Asal Sekolah Judge 01 Judge 02 Judge 03 Total ScoreBastianggaÎncă nu există evaluări
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Minoxidil Use in Dermatology, Side Effects and Recent PatentsDocument12 paginiMinoxidil Use in Dermatology, Side Effects and Recent PatentsBastianggaÎncă nu există evaluări
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- AutopsyDocument207 paginiAutopsyBastianggaÎncă nu există evaluări
- Autopsy in Islam and Current Practice in Arab Muslim Countries HistoryDocument4 paginiAutopsy in Islam and Current Practice in Arab Muslim Countries HistoryBastianggaÎncă nu există evaluări
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- Notes For Perioperative NursingDocument5 paginiNotes For Perioperative NursingNey JuneÎncă nu există evaluări
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- Self Applied Topical Fluorides ClassDocument23 paginiSelf Applied Topical Fluorides ClassultraswamyÎncă nu există evaluări
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Perceptions and Beliefs Regarding Caesarean Section Among Pregnant Women Receiving Antenatal Care at Ishaka Adventist HospitalDocument12 paginiPerceptions and Beliefs Regarding Caesarean Section Among Pregnant Women Receiving Antenatal Care at Ishaka Adventist HospitalKIU PUBLICATION AND EXTENSIONÎncă nu există evaluări
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- ICRA Form v08.07Document5 paginiICRA Form v08.07Indra Juang Putra HarefaÎncă nu există evaluări
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- Lymphatic System NotesDocument4 paginiLymphatic System Notestaccxo14Încă nu există evaluări
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- MCQ Sick NewbornDocument21 paginiMCQ Sick NewbornprabhatÎncă nu există evaluări
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Management of AUB in A Bicornuate Uterus - Endometrial Ablation in A CompDocument1 paginăManagement of AUB in A Bicornuate Uterus - Endometrial Ablation in A Comptipu42Încă nu există evaluări
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- Pediatric Pulmonology 2021, Dell'ortoDocument8 paginiPediatric Pulmonology 2021, Dell'ortoRadu CiprianÎncă nu există evaluări
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- National Clinical Guideline No. 5 Clinical Handover Nov2014Document306 paginiNational Clinical Guideline No. 5 Clinical Handover Nov2014Ahmad JuliadiÎncă nu există evaluări
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- The Aging Voice: Presented by Anastasia Serbalik Presented To Rebecca L. Gould, MSC, CCC-SLPDocument32 paginiThe Aging Voice: Presented by Anastasia Serbalik Presented To Rebecca L. Gould, MSC, CCC-SLPAtri AmmuluÎncă nu există evaluări
- Final Year QN Papers (1990-2017)Document37 paginiFinal Year QN Papers (1990-2017)vardhan hhh100% (4)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- 024344Document6 pagini024344Aravind DesaiÎncă nu există evaluări
- Posterior Capsular OpacityDocument3 paginiPosterior Capsular OpacityRandy FerdianÎncă nu există evaluări
- Neck, Part 1: With Dr. Craig CanbyDocument36 paginiNeck, Part 1: With Dr. Craig CanbyMalikkahÎncă nu există evaluări
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (345)
- Pathology Laboratory in AhmedabadDocument73 paginiPathology Laboratory in Ahmedabaddivyesh_sharma_20% (1)
- PIHDocument12 paginiPIHAnonymous pt6eA0100% (1)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- Role Play: Gastritic: Make An A VoitmentDocument3 paginiRole Play: Gastritic: Make An A VoitmentGita MirnawatiÎncă nu există evaluări
- OR AppendixDocument9 paginiOR AppendixDan HizonÎncă nu există evaluări
- Episiotomy & Episiorrhaphy: Dr. SumayyaDocument35 paginiEpisiotomy & Episiorrhaphy: Dr. SumayyaMuhammad IbrahimÎncă nu există evaluări
- Sociology of Health and Illness: Fergusos@grinnell - EduDocument18 paginiSociology of Health and Illness: Fergusos@grinnell - EduRanchuJoseÎncă nu există evaluări
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- NSO Monthly Report FormDocument5 paginiNSO Monthly Report Formrose_almonteÎncă nu există evaluări
- Definition, History, Scope and Nature of Legal MedicineDocument22 paginiDefinition, History, Scope and Nature of Legal Medicinesescuzar100% (1)
- Ellen Hill: Master of Public Health in Nutritional SciencesDocument2 paginiEllen Hill: Master of Public Health in Nutritional Sciencesapi-434483502Încă nu există evaluări
- Health Family Welfare 3Document225 paginiHealth Family Welfare 3Gopala Sundararaj SÎncă nu există evaluări
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Acog Practice Bulletin: Inherited Thrombophilias in PregnancyDocument17 paginiAcog Practice Bulletin: Inherited Thrombophilias in PregnancyDora Maria Guadamuz MoralesÎncă nu există evaluări
- Emergency Room Care-What Older Persons and Caregivers Need To KnowDocument14 paginiEmergency Room Care-What Older Persons and Caregivers Need To KnowshoriatÎncă nu există evaluări
- The Health Care ProcessDocument6 paginiThe Health Care ProcessLineveange B LiuqnanamÎncă nu există evaluări
- المصادر المعتمدة في فرع تمريض الام والوليدDocument6 paginiالمصادر المعتمدة في فرع تمريض الام والوليدمنتظر عبدالعظيم عبدالله حميدÎncă nu există evaluări
- Positioning QuestionsDocument5 paginiPositioning QuestionsShara SampangÎncă nu există evaluări
- Research Proposal o NishaDocument14 paginiResearch Proposal o NishaNishaThakuri100% (1)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)