S-ar putea să vă placă și
- 2023 OB/GYN Coding Manual: Components of Correct CodingDe la Everand2023 OB/GYN Coding Manual: Components of Correct CodingÎncă nu există evaluări
- Handbook of Current and Novel Protocols for the Treatment of InfertilityDe la EverandHandbook of Current and Novel Protocols for the Treatment of InfertilityMichael H. DahanÎncă nu există evaluări
- Acid Base Tutorial - University of ConnecticutDocument47 paginiAcid Base Tutorial - University of ConnecticutClaudioGutierrezFrausto80% (5)
- Peds and Med OSCE GuideDocument8 paginiPeds and Med OSCE GuideAbdulÎncă nu există evaluări
- ACOG Practice Bulletin No 99 Management of 39 PDFDocument26 paginiACOG Practice Bulletin No 99 Management of 39 PDFhkdawnwongÎncă nu există evaluări
- Low Grade Glioma Treatment and PrognosisDocument5 paginiLow Grade Glioma Treatment and PrognosisDiana MitreaÎncă nu există evaluări
- SkeletaxrayDocument144 paginiSkeletaxrayradiologgÎncă nu există evaluări
- Hiperplasia EndometrialDocument12 paginiHiperplasia EndometrialJulián LópezÎncă nu există evaluări
- Medical Imaging TechniquesDocument96 paginiMedical Imaging TechniquesNazia WasimÎncă nu există evaluări
- Training in Obstetrics and Gynaecology - Ippokratis SarrisDocument4 paginiTraining in Obstetrics and Gynaecology - Ippokratis Sarriszuxifoho0% (1)
- Star Primer 2014 InvitationDocument4 paginiStar Primer 2014 InvitationBhavik ChopdaÎncă nu există evaluări
- Post Coital BleedingDocument8 paginiPost Coital BleedingMutiara SwÎncă nu există evaluări
- 1stprize CR Auditpostercomp C Reid 2015Document1 pagină1stprize CR Auditpostercomp C Reid 2015webber_denzÎncă nu există evaluări
- 1-Introduction To RadiologyDocument15 pagini1-Introduction To RadiologyMuhammed Maryam ometereÎncă nu există evaluări
- Nuclear Medicine GuideDocument3 paginiNuclear Medicine GuidejeffsunilÎncă nu există evaluări
- EAU ESUR ESTRO SIOG Guidelines On Prostate Cancer Large Text V2Document145 paginiEAU ESUR ESTRO SIOG Guidelines On Prostate Cancer Large Text V2DellaÎncă nu există evaluări
- Ovarian Ultrasonography and Follow of Estrus in The Bitch and QueenDocument8 paginiOvarian Ultrasonography and Follow of Estrus in The Bitch and QueenTere GarzónÎncă nu există evaluări
- Evaluation and Routine Testing in Medical Imaging DepartmentsDocument18 paginiEvaluation and Routine Testing in Medical Imaging DepartmentsRankie Choi100% (1)
- Ovarian CystsDocument15 paginiOvarian Cystserna safriyantiÎncă nu există evaluări
- Breast MRI Teaching Atlas by Richard Ha, Christopher E. Comstock, Elizabeth A. Morris (Eds.)Document65 paginiBreast MRI Teaching Atlas by Richard Ha, Christopher E. Comstock, Elizabeth A. Morris (Eds.)geovanaÎncă nu există evaluări
- Comparison of Serum Microseminoprotein-Beta (MSMB) With Total Prostate Specific Antigen (TPSA) in The Diagnosis of Prostate Cancer in African MenDocument7 paginiComparison of Serum Microseminoprotein-Beta (MSMB) With Total Prostate Specific Antigen (TPSA) in The Diagnosis of Prostate Cancer in African MenInternational Journal of Innovative Science and Research TechnologyÎncă nu există evaluări
- Ad en Om Yo SisDocument6 paginiAd en Om Yo SisMariaa EndahhÎncă nu există evaluări
- Table 4.1 AFS Classifi Cation System (: The Embryological-Clinical Classifi CationDocument111 paginiTable 4.1 AFS Classifi Cation System (: The Embryological-Clinical Classifi CationArya Syafaromania RachmaÎncă nu există evaluări
- Birads 2013Document6 paginiBirads 2013Citlaly RojasÎncă nu există evaluări
- GA by Ultrasound SOGCDocument11 paginiGA by Ultrasound SOGCBrendaÎncă nu există evaluări
- 2022 Mendoza Eligibility CriteriaDocument21 pagini2022 Mendoza Eligibility CriteriaТатьяна ТутченкоÎncă nu există evaluări
- Prevalence and Factors Associated With Routine Medical Checkup Among Patients Attending Masaka Regional Referral Hospital, UgandaDocument9 paginiPrevalence and Factors Associated With Routine Medical Checkup Among Patients Attending Masaka Regional Referral Hospital, UgandaIJAR JOURNALÎncă nu există evaluări
- DR Poli Obs Ii Mug 01.03.19Document22 paginiDR Poli Obs Ii Mug 01.03.19mughanÎncă nu există evaluări
- Endometriosis With Salpingitis Simulating Acute AppendicitisDocument20 paginiEndometriosis With Salpingitis Simulating Acute AppendicitisWyendae CliquersÎncă nu există evaluări
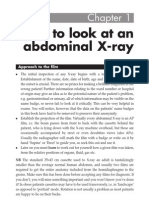
- How To Read An Abdominal XrayDocument38 paginiHow To Read An Abdominal Xraytwentyjazzfunkgreats3055100% (1)
- 62 Colposcopy StandardsDocument73 pagini62 Colposcopy Standardsrijal mahdiy pÎncă nu există evaluări
- Testicular Cancer Fact Sheet PDFDocument2 paginiTesticular Cancer Fact Sheet PDFRandaÎncă nu există evaluări
- Evaluation of Right Side Foetal Myocardial Performance Index in Pregestational and Gestational Diabetes MellitusDocument7 paginiEvaluation of Right Side Foetal Myocardial Performance Index in Pregestational and Gestational Diabetes MellitusGabyliz Gonzalez CastilloÎncă nu există evaluări
- Cervical Spine Trauma Imaging GuideDocument25 paginiCervical Spine Trauma Imaging GuideComagaÎncă nu există evaluări
- Physics Lecture on Mammography X-Ray SystemsDocument42 paginiPhysics Lecture on Mammography X-Ray SystemsLajja Parikh PatelÎncă nu există evaluări
- ICRP 23 Reference ManDocument504 paginiICRP 23 Reference ManFlávio Augusto SoaresÎncă nu există evaluări
- Detecting Ectopic Pregnancies with UltrasoundDocument30 paginiDetecting Ectopic Pregnancies with UltrasoundgarciajulioÎncă nu există evaluări
- Review of Medical Microbiology and Immunology 17th Edition (Medicalstudyzone - Com)Document1.016 paginiReview of Medical Microbiology and Immunology 17th Edition (Medicalstudyzone - Com)FaizÎncă nu există evaluări
- Anesthesia For Hysteroscopy: A Comparison of General and Spinal AnesthesiaDocument7 paginiAnesthesia For Hysteroscopy: A Comparison of General and Spinal AnesthesiaIJAR JOURNALÎncă nu există evaluări
- Ul Css Lung CovidDocument7 paginiUl Css Lung CovidJC 89Încă nu există evaluări
- Preterm+Prelabour+Rupture+of+the+Membranes Sept2015Document12 paginiPreterm+Prelabour+Rupture+of+the+Membranes Sept2015molenÎncă nu există evaluări
- Repro & Endo 3Document26 paginiRepro & Endo 3abdulÎncă nu există evaluări
- Senior Radiographer Nuclear MedicineDocument1 paginăSenior Radiographer Nuclear Medicinetafi66Încă nu există evaluări
- Hamerlynck2018 Article FertilityOutcomeAfterTreatmentDocument7 paginiHamerlynck2018 Article FertilityOutcomeAfterTreatmentMahida El shafiÎncă nu există evaluări
- Fetal Biometry and Growth ChartsDocument27 paginiFetal Biometry and Growth ChartsnellieauthorÎncă nu există evaluări
- Nuclear Medicine Inc.'s Iodine Value Chain AnalysisDocument6 paginiNuclear Medicine Inc.'s Iodine Value Chain AnalysisPrashant NagpureÎncă nu există evaluări
- Nuclear Medicine Tehnologist or Lead Nuclear Medicine TechnologiDocument2 paginiNuclear Medicine Tehnologist or Lead Nuclear Medicine Technologiapi-78955179Încă nu există evaluări
- Vaginal Vault ProlapseDocument9 paginiVaginal Vault ProlapseOanaÎncă nu există evaluări
- SAUDI BOARD FINAL CLINICAL EXAM OF GENERAL SURGERYDocument6 paginiSAUDI BOARD FINAL CLINICAL EXAM OF GENERAL SURGERYMohammed S. Al GhamdiÎncă nu există evaluări
- Lung Cyst Case ReportDocument64 paginiLung Cyst Case ReportJavaid Khan100% (1)
- Germ Cell TumoursDocument32 paginiGerm Cell Tumoursapi-3705046Încă nu există evaluări
- Barium StudiesDocument16 paginiBarium StudiesRuby Dela RamaÎncă nu există evaluări
- Screening Case Study Exercises - Hannah TurnerDocument4 paginiScreening Case Study Exercises - Hannah Turnerapi-457299309Încă nu există evaluări
- Clinical Guideline: Prelabour Rupture of The Membranes (PROM) 37 Weeks Clinical GuidelineDocument10 paginiClinical Guideline: Prelabour Rupture of The Membranes (PROM) 37 Weeks Clinical GuidelineUtomo BudidarmoÎncă nu există evaluări
- ISUOG - Fetal Nervous System ExaminationDocument8 paginiISUOG - Fetal Nervous System ExaminationAzucenaÎncă nu există evaluări
- CT ANGIOGRAPHY - DETAILED IMAGES OF BLOOD VESSELSDocument1 paginăCT ANGIOGRAPHY - DETAILED IMAGES OF BLOOD VESSELSsreejithÎncă nu există evaluări
- Gui322cpg1504e2 PDFDocument15 paginiGui322cpg1504e2 PDFieo100% (1)
- Safety of Radiographic Imaging During Pregnancy - American Family PhysicianDocument7 paginiSafety of Radiographic Imaging During Pregnancy - American Family PhysicianDuddy Ari HardiantoÎncă nu există evaluări
- Basic Considerations in Nuclear MedicineDocument12 paginiBasic Considerations in Nuclear Medicinechberg13Încă nu există evaluări
- Transabdominal and Transvaginal Ultrasound of the UterusDocument68 paginiTransabdominal and Transvaginal Ultrasound of the UterusEsraa AlmassriÎncă nu există evaluări
- PostDocument8 paginiPostSultan AlexandruÎncă nu există evaluări
- C.Sordellii Contamination: Phagocytes in Endometrium Proinflamatory Cytokines Release Weaken Innate Immune SystemDocument1 paginăC.Sordellii Contamination: Phagocytes in Endometrium Proinflamatory Cytokines Release Weaken Innate Immune Systemaldea_844577109Încă nu există evaluări
- Comparative Hematology Values in MammalsDocument30 paginiComparative Hematology Values in MammalsSultan AlexandruÎncă nu există evaluări
- Bits&Bytes - Surviving Morning Rounds 2012Document323 paginiBits&Bytes - Surviving Morning Rounds 2012D. BarÎncă nu există evaluări
- Chapter 10 - The Mature ErythrocyteDocument55 paginiChapter 10 - The Mature ErythrocyteSultan AlexandruÎncă nu există evaluări
- MasteringthmedicineeBoardsandClinincalExaminationsinInternalMedicine Part1Document814 paginiMasteringthmedicineeBoardsandClinincalExaminationsinInternalMedicine Part1metallic_ghostreconÎncă nu există evaluări
- Chapter 48 - Acquired Hemolytic Anemias Resulting From DirecDocument22 paginiChapter 48 - Acquired Hemolytic Anemias Resulting From DirecSultan AlexandruÎncă nu există evaluări
- MotdDocument1 paginăMotdIrinel LoghinÎncă nu există evaluări
- Chapter 3 - ImmunodiagnosisDocument37 paginiChapter 3 - ImmunodiagnosisSultan AlexandruÎncă nu există evaluări
- APPENDIX A-Normal Values in HumansDocument22 paginiAPPENDIX A-Normal Values in HumansSultan AlexandruÎncă nu există evaluări
- GI Practice Review - 2nd Edition - ABRThomson 2012Document744 paginiGI Practice Review - 2nd Edition - ABRThomson 2012Sultan AlexandruÎncă nu există evaluări
- Achieving Excellence in The OSCE Part 1Document409 paginiAchieving Excellence in The OSCE Part 1Sultan AlexandruÎncă nu există evaluări
- GI Practice Review - 2nd Edition - ABRThomson 2012Document744 paginiGI Practice Review - 2nd Edition - ABRThomson 2012Sultan AlexandruÎncă nu există evaluări
- Achieving Excellence in The OSCE Part 2Document465 paginiAchieving Excellence in The OSCE Part 2Sultan AlexandruÎncă nu există evaluări
- Comparative Hematology Values in MammalsDocument30 paginiComparative Hematology Values in MammalsSultan AlexandruÎncă nu există evaluări
- Cytopathology of Infectious DiseasesDocument404 paginiCytopathology of Infectious DiseasesSultan AlexandruÎncă nu există evaluări
- RELEASEDocument22 paginiRELEASEsuwandaniÎncă nu există evaluări
- Bits&Bytes - Surviving Morning Rounds 2012Document323 paginiBits&Bytes - Surviving Morning Rounds 2012D. BarÎncă nu există evaluări
- Tauras Beko Tv2k Ag Bk2 20 St92195 Stv2248 Chassis K Bomann Ctv577v Chassis Pm2tv2k SCHDocument1 paginăTauras Beko Tv2k Ag Bk2 20 St92195 Stv2248 Chassis K Bomann Ctv577v Chassis Pm2tv2k SCHtodorloncarskiÎncă nu există evaluări
- MEDDICDocument5.328 paginiMEDDICSultan AlexandruÎncă nu există evaluări
- LicenseDocument2 paginiLicenseSultan AlexandruÎncă nu există evaluări
- ReadmeplDocument3 paginiReadmeplSultan AlexandruÎncă nu există evaluări
- ReadmeDocument1 paginăReadmeZalán HorváthÎncă nu există evaluări
- SpectcammenuDocument1 paginăSpectcammenuomucz95Încă nu există evaluări
- English ProficiencyDocument3 paginiEnglish ProficiencySultan AlexandruÎncă nu există evaluări
- Professional Guid8e To Signs and Symptoms 5th Ed 2007 WWDocument2.044 paginiProfessional Guid8e To Signs and Symptoms 5th Ed 2007 WWSultan AlexandruÎncă nu există evaluări
- Heart Sounds PDFDocument38 paginiHeart Sounds PDFZennon Blaze ArceusÎncă nu există evaluări
- Biology Weekly Worksheet g7s2pb Transport in HumansDocument5 paginiBiology Weekly Worksheet g7s2pb Transport in HumansD'ferti AnggraeniÎncă nu există evaluări
- Quick Guide, Volume 1 - 453562006191b - en-US PDFDocument82 paginiQuick Guide, Volume 1 - 453562006191b - en-US PDFIvan CvasniucÎncă nu există evaluări
- Reymart Baguio A. Iii Bsed-Science Module 4 - Fluids and Transport Module Assessment Critical Thinking QuestionsDocument13 paginiReymart Baguio A. Iii Bsed-Science Module 4 - Fluids and Transport Module Assessment Critical Thinking QuestionsReymart Anga Baguio IIÎncă nu există evaluări
- 1.8.2 HandoutDocument4 pagini1.8.2 Handoutkhushisarfraz123Încă nu există evaluări
- Oral Revalida ReviewerDocument10 paginiOral Revalida RevieweranneÎncă nu există evaluări
- Robbins Basic Pathology 9th Edition Kumar Test BankDocument6 paginiRobbins Basic Pathology 9th Edition Kumar Test Bankvolitiveacrosporedur100% (24)
- POCUS Sobrecarga 2022Document13 paginiPOCUS Sobrecarga 2022tavo570Încă nu există evaluări
- Exercise 15 Cardiovascular SystDocument6 paginiExercise 15 Cardiovascular Systholie madroneroÎncă nu există evaluări
- Animal PhysiologyDocument104 paginiAnimal PhysiologyClara MaeÎncă nu există evaluări
- Outline of Anatomy and Physiology (Semifinal-Final)Document8 paginiOutline of Anatomy and Physiology (Semifinal-Final)Jhason John J. CabigonÎncă nu există evaluări
- Cambridge International AS & A Level: Biology 9700/13Document20 paginiCambridge International AS & A Level: Biology 9700/13Mighty Warrior GSRÎncă nu există evaluări
- Cardiology Summary PDFDocument62 paginiCardiology Summary PDFSyamsuriWahyuÎncă nu există evaluări
- Free PPT Templates for Modern PresentationsDocument48 paginiFree PPT Templates for Modern PresentationsDella Puspita SariÎncă nu există evaluări
- Design and Implementation of Bioamplifier For Portable ECG DeviceDocument19 paginiDesign and Implementation of Bioamplifier For Portable ECG Devicej4everÎncă nu există evaluări
- Cardiovascular MCQsDocument17 paginiCardiovascular MCQsRamadan PhysiologyÎncă nu există evaluări
- Science - G9 - Week 2 (Lessons-4-6)Document46 paginiScience - G9 - Week 2 (Lessons-4-6)Rhyan Zero-four BaluyutÎncă nu există evaluări
- Interpretation Chest X RayDocument127 paginiInterpretation Chest X RayVimal NishadÎncă nu există evaluări
- Anatomi Kardio PDFDocument49 paginiAnatomi Kardio PDFDestrini Anjani LandaÎncă nu există evaluări
- Biol 1700 - Assignment 2Document16 paginiBiol 1700 - Assignment 2api-456450673100% (1)
- Hear T: 12.1 Functions of The HeartDocument9 paginiHear T: 12.1 Functions of The HeartBeah Marie AlisosoÎncă nu există evaluări
- Test Bank For Ekg Plain and Simple 4th Edition by Ellis Chapters 12-15-18 Not IncludedDocument11 paginiTest Bank For Ekg Plain and Simple 4th Edition by Ellis Chapters 12-15-18 Not Includedcanebrutalfniy66Încă nu există evaluări
- ME Sci 9 Q1 0103 PSDocument18 paginiME Sci 9 Q1 0103 PScassiopeia bianca sartigaÎncă nu există evaluări
- Autopsy: Forensic Medicine & Toxicology, NMCDocument106 paginiAutopsy: Forensic Medicine & Toxicology, NMCAiman sadiq shahÎncă nu există evaluări
- Cardiology: Enema - Invasive But Does Not Use Sterile TechniqueDocument6 paginiCardiology: Enema - Invasive But Does Not Use Sterile TechniqueGe MiniÎncă nu există evaluări
- Cardiovascular AssessmentDocument21 paginiCardiovascular AssessmentRhitzle AnnÎncă nu există evaluări
- Littmann Cardiac AuscultationDocument1 paginăLittmann Cardiac AuscultationSri Wahyuni100% (1)
- Dr. Mohammad Shaikhani. Sulaimani University, College of Medicine. Sulaimanya-Iraqi KurdistanDocument51 paginiDr. Mohammad Shaikhani. Sulaimani University, College of Medicine. Sulaimanya-Iraqi KurdistanHNINÎncă nu există evaluări
- KP 1.3.2.1 Aktivitas Mekanik Jantung (2 Jam)Document68 paginiKP 1.3.2.1 Aktivitas Mekanik Jantung (2 Jam)Try MutiaraÎncă nu există evaluări