S-ar putea să vă placă și
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5795)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1091)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Mergers and Acquisitions of Hindalco and NovelisDocument35 paginiMergers and Acquisitions of Hindalco and Novelisashukejriwal007Încă nu există evaluări
- Ijel - Mickey's Christmas Carol A Derivation That IDocument6 paginiIjel - Mickey's Christmas Carol A Derivation That ITJPRC PublicationsÎncă nu există evaluări
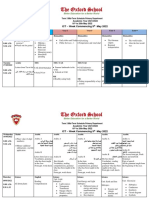
- Term 3 Mid-Term Assessment ScheduleDocument9 paginiTerm 3 Mid-Term Assessment ScheduleRabia MoeedÎncă nu există evaluări
- Voloxal TabletsDocument9 paginiVoloxal Tabletselcapitano vegetaÎncă nu există evaluări
- Is 456 - 2016 4th Amendment Plain and Reinforced Concrete - Code of Practice - Civil4MDocument3 paginiIs 456 - 2016 4th Amendment Plain and Reinforced Concrete - Code of Practice - Civil4Mvasudeo_ee0% (1)
- Progress Test 1 Units 1-6: Exercise 1 Personal InformationDocument3 paginiProgress Test 1 Units 1-6: Exercise 1 Personal InformationLuis Villaverde VerasteguiÎncă nu există evaluări
- Causes of Traffic Congestions in Urban AreaDocument9 paginiCauses of Traffic Congestions in Urban AreaaqilahÎncă nu există evaluări
- NameDocument16 paginiNameAfro BertÎncă nu există evaluări
- Dina Iordanova - Women in Balkan Cinema, Surviving On The MarginsDocument17 paginiDina Iordanova - Women in Balkan Cinema, Surviving On The MarginsimparatulverdeÎncă nu există evaluări
- Warm Pretend Lead Line Cater Resist Provide Reflect Anticipate Advertise Range Sentence AccessDocument24 paginiWarm Pretend Lead Line Cater Resist Provide Reflect Anticipate Advertise Range Sentence AccessJacinto Leite Aquino RêgoÎncă nu există evaluări
- Health COX's Monthly Dashboard - 2023 NovDocument4 paginiHealth COX's Monthly Dashboard - 2023 Novcox mamÎncă nu există evaluări
- Acctg 604 Basic Framework of Mas Cost Managemet PDFDocument55 paginiAcctg 604 Basic Framework of Mas Cost Managemet PDFKookie100% (1)
- RMJ PDF Min v2 PDFDocument17 paginiRMJ PDF Min v2 PDFAli AhmadÎncă nu există evaluări
- Karling Aguilera-Fort ResumeDocument4 paginiKarling Aguilera-Fort Resumeapi-3198760590% (1)
- 50 Interview Questions For Adryenn AshleyDocument5 pagini50 Interview Questions For Adryenn AshleyAdryenn AshleyÎncă nu există evaluări
- FIDP Business Ethics and Social Responsibility PDFDocument7 paginiFIDP Business Ethics and Social Responsibility PDFRachell Mae Bondoc 1Încă nu există evaluări
- Quamet1 - CM6Document10 paginiQuamet1 - CM6Bob ReymartÎncă nu există evaluări
- Agostinis Et Al-2011-CA - A Cancer Journal For CliniciansDocument32 paginiAgostinis Et Al-2011-CA - A Cancer Journal For CliniciansKauniIsaacÎncă nu există evaluări
- The SacrificeDocument3 paginiThe SacrificeRoseann Hidalgo ZimaraÎncă nu există evaluări
- Objectives: A. Identify The Reasons For Keeping Business Records and B. Perform Key Bookkeeping TaskDocument11 paginiObjectives: A. Identify The Reasons For Keeping Business Records and B. Perform Key Bookkeeping TaskMarife CulabaÎncă nu există evaluări
- 08 03 Runge-Kutta 2nd Order MethodDocument11 pagini08 03 Runge-Kutta 2nd Order MethodJohn Bofarull GuixÎncă nu există evaluări
- Survey Questionnaire FsDocument6 paginiSurvey Questionnaire FsHezell Leah ZaragosaÎncă nu există evaluări
- 158 Carino vs. CADocument2 pagini158 Carino vs. CAFrancesca Isabel Montenegro67% (3)
- Distosia BahuDocument185 paginiDistosia BahuAdith Fileanugraha100% (1)
- Theatre History TimelineDocument7 paginiTheatre History TimelineCzar Paulo Dabon100% (2)
- RB September 2014 The One Thing Kekuatan Fokus Untuk Mendorong ProduktivitasDocument2 paginiRB September 2014 The One Thing Kekuatan Fokus Untuk Mendorong ProduktivitasRifat TaopikÎncă nu există evaluări
- Arts 9 M1 Q3 1Document15 paginiArts 9 M1 Q3 1Gina GalvezÎncă nu există evaluări
- Reaction Paper PoliticsDocument1 paginăReaction Paper PoliticsDenise Jim GalantaÎncă nu există evaluări
- Cost Accounting and Management Essentials You Always Wanted To Know: 4th EditionDocument21 paginiCost Accounting and Management Essentials You Always Wanted To Know: 4th EditionVibrant Publishers100% (1)
- Classroom of The Elite Year 2 Volume 4Document49 paginiClassroom of The Elite Year 2 Volume 4ANANT GUPTAÎncă nu există evaluări