S-ar putea să vă placă și
- Association of Empty Sella and Neuroendocrine Disorders in Childhood 1995Document5 paginiAssociation of Empty Sella and Neuroendocrine Disorders in Childhood 1995Paúl Otañez MolinaÎncă nu există evaluări
- 123I-MIBG Cutoff Points for PDDocument8 pagini123I-MIBG Cutoff Points for PDPUIGCOZARÎncă nu există evaluări
- JCO 2019 MRD Phéno Myélome PDFDocument20 paginiJCO 2019 MRD Phéno Myélome PDFTony HuynhÎncă nu există evaluări
- Idiopathic Growth Hormone DeficiencyDocument8 paginiIdiopathic Growth Hormone Deficiencyrenno85Încă nu există evaluări
- FABDocument4 paginiFABNadine SmithÎncă nu există evaluări
- D2, D3 ReceptroiDocument8 paginiD2, D3 ReceptroiBrain RunnerÎncă nu există evaluări
- 52 58 Semenko V.V. ENDOTHELINE 1s DYNAMICS IN NON PROLIFERATIVE DIABETIC RETINOPATHY AND ITS CORRECTION WITH LARGININE PDFDocument7 pagini52 58 Semenko V.V. ENDOTHELINE 1s DYNAMICS IN NON PROLIFERATIVE DIABETIC RETINOPATHY AND ITS CORRECTION WITH LARGININE PDFTito saragihÎncă nu există evaluări
- Correlation Between Diabetic Cognitive Impairment and Diabetic Retinopathy in Patients With T2DM by 1H-MRSDocument7 paginiCorrelation Between Diabetic Cognitive Impairment and Diabetic Retinopathy in Patients With T2DM by 1H-MRSppdsretinaÎncă nu există evaluări
- Shymanskaya Comparison of 18F Fluoroethyltyrosine PET and 23na MRI in GliomasDocument10 paginiShymanskaya Comparison of 18F Fluoroethyltyrosine PET and 23na MRI in GliomasAlfonso LemaÎncă nu există evaluări
- Jurnal Mata 2Document30 paginiJurnal Mata 2Reza AryantiÎncă nu există evaluări
- 2019-Dfsdda SDocument7 pagini2019-Dfsdda SAhmet KaragozÎncă nu există evaluări
- SANCHEZ GONZALEZ FEDERICO Type II Focal Cortical Dysplasia - Electroclinical Study and Surgical Outcome in 31 Pediatric Patients 2013Document9 paginiSANCHEZ GONZALEZ FEDERICO Type II Focal Cortical Dysplasia - Electroclinical Study and Surgical Outcome in 31 Pediatric Patients 2013Federicos Sánchez GonzálezÎncă nu există evaluări
- GRIN2A-related Disorders Genotype and Functional Consequence Predict Phenotype Strehlow 2018Document13 paginiGRIN2A-related Disorders Genotype and Functional Consequence Predict Phenotype Strehlow 2018cicasmileÎncă nu există evaluări
- NIMS PDF 2022 Prospectus FinalDocument15 paginiNIMS PDF 2022 Prospectus Finalmaaddy001Încă nu există evaluări
- Arnaldi 2017Document10 paginiArnaldi 2017Jaime AguilarÎncă nu există evaluări
- noz124Document10 pagininoz124albertoÎncă nu există evaluări
- Reljanovic Et Al. - 1999 - Treatment of Diabetic Polyneuropathy With The Antioxidant Thioctic Acid (Alpha-Lipoic Acid) A Two Year Multi Center Randomized DoubleDocument9 paginiReljanovic Et Al. - 1999 - Treatment of Diabetic Polyneuropathy With The Antioxidant Thioctic Acid (Alpha-Lipoic Acid) A Two Year Multi Center Randomized DoubleJay LawÎncă nu există evaluări
- F-FDG Pet/Ct and I-Metaiodobenzylguanidine Imaging in High-Risk Neuroblastoma: Diagnostic Comparison and Survival AnalysisDocument7 paginiF-FDG Pet/Ct and I-Metaiodobenzylguanidine Imaging in High-Risk Neuroblastoma: Diagnostic Comparison and Survival AnalysisManos PanagiotidisÎncă nu există evaluări
- The Landscape of Epilepsy-Related GATOR1 Variants Baldassari 2019Document11 paginiThe Landscape of Epilepsy-Related GATOR1 Variants Baldassari 2019cicasmileÎncă nu există evaluări
- Articulo Fisio 3Document7 paginiArticulo Fisio 3Oumaima Ahaddouch ChiniÎncă nu există evaluări
- Extrapyramid SynDocument7 paginiExtrapyramid SynZahra Namika AiharaÎncă nu există evaluări
- Basal Gangila CahngesDocument12 paginiBasal Gangila CahngesJakkani RavikanthÎncă nu există evaluări
- Incidencia Clinica Demencia Frontal LeidoDocument7 paginiIncidencia Clinica Demencia Frontal LeidoFelipeWebster CorderoÎncă nu există evaluări
- IDH1 and IDH2 Mutations in Lung Adenocarcinomas EvDocument9 paginiIDH1 and IDH2 Mutations in Lung Adenocarcinomas EvNathur IdrisÎncă nu există evaluări
- Molecules 24 03221Document12 paginiMolecules 24 03221Ignacio Pérez-VictoriaÎncă nu există evaluări
- Blink ReflexDocument5 paginiBlink ReflexRyan TanÎncă nu există evaluări
- Doenças RarasDocument11 paginiDoenças RarasJean CarlosÎncă nu există evaluări
- Chi 2019Document9 paginiChi 2019docadax848Încă nu există evaluări
- BJR 83 590Document6 paginiBJR 83 590Paulo Henrique Vizoná de OliveiraÎncă nu există evaluări
- Frontiers Nidhi Publication in DMDDocument9 paginiFrontiers Nidhi Publication in DMDnidhideepu94Încă nu există evaluări
- Diffuse Leptomeningeal Neuroepithelial TumorDocument9 paginiDiffuse Leptomeningeal Neuroepithelial TumorAdelina FeitosaÎncă nu există evaluări
- Dopamine Receptor Subtypes, Physiology and Pharmacology - New Ligands and Concepts in SchizophreniaDocument17 paginiDopamine Receptor Subtypes, Physiology and Pharmacology - New Ligands and Concepts in SchizophreniaolivukovicÎncă nu există evaluări
- Kaya - GD-15Document6 paginiKaya - GD-15SzendeÎncă nu există evaluări
- Treatment of Delirium With Quetiapine: One Personal Copy May Be PrintedDocument3 paginiTreatment of Delirium With Quetiapine: One Personal Copy May Be PrintedMahmoud WardÎncă nu există evaluări
- Labmed31 0383Document4 paginiLabmed31 0383ushakÎncă nu există evaluări
- Retinal Nerve Fiber Layer and Ganglion Cell Complex Thickness in Patients With Type 2 Diabetes Mellitus Original ArticleDocument2 paginiRetinal Nerve Fiber Layer and Ganglion Cell Complex Thickness in Patients With Type 2 Diabetes Mellitus Original ArticledrblurryfaceÎncă nu există evaluări
- Restrictive Cardiomyopathy Case ReportDocument7 paginiRestrictive Cardiomyopathy Case ReportLADY JOWAHER ALLASÎncă nu există evaluări
- 1 s2.0 S0272638622008216 MainDocument3 pagini1 s2.0 S0272638622008216 MainhernanÎncă nu există evaluări
- SPECT/CT fusion clarifies uncertain cancer fociDocument11 paginiSPECT/CT fusion clarifies uncertain cancer fociAxelSesT MtzÎncă nu există evaluări
- Evaluation of The NINCDS-ADRDA CriteriaDocument6 paginiEvaluation of The NINCDS-ADRDA Criteriadogstar23Încă nu există evaluări
- Makale Neo-Adma - Eng V2Document12 paginiMakale Neo-Adma - Eng V2Thomas LeonÎncă nu există evaluări
- Stadio 2019Document5 paginiStadio 2019FernandoÎncă nu există evaluări
- Craniopharyngioma: Analysis of Factors That Affect The OutcomeDocument5 paginiCraniopharyngioma: Analysis of Factors That Affect The OutcomeRiri KumalaÎncă nu există evaluări
- Ugc Carelist Journals 22novDocument7 paginiUgc Carelist Journals 22novnaresh kotraÎncă nu există evaluări
- Callega Gero Et Al. 2011. Neuroimaging Findings in Patient Series With MucopolysaccharidosisDocument7 paginiCallega Gero Et Al. 2011. Neuroimaging Findings in Patient Series With MucopolysaccharidosisBoÎncă nu există evaluări
- Diagnosis of Aerogenic Dyslipidemia in Primary Care in SP 2020 AtherosclerosDocument2 paginiDiagnosis of Aerogenic Dyslipidemia in Primary Care in SP 2020 Atherosclerosmibelvar87Încă nu există evaluări
- Jurnalparkinson 2Document10 paginiJurnalparkinson 2Vita SariÎncă nu există evaluări
- Clinical Characteristics of CyclodeviationDocument7 paginiClinical Characteristics of Cyclodeviationcarlosalladoa0% (1)
- Fingolimod Nejm Pelletier2012 PDFDocument9 paginiFingolimod Nejm Pelletier2012 PDFCESAR AUGUSTO CARVAJAL RENDONÎncă nu există evaluări
- Predictors For Diabetic Retinopathy in Normoalbuminuric People With Type 2 Diabetes MellitusDocument6 paginiPredictors For Diabetic Retinopathy in Normoalbuminuric People With Type 2 Diabetes MellitusdrheriÎncă nu există evaluări
- Distinguishing Dementia with Lewy Bodies and Alzheimer's Disease Using MRI and SPECTDocument6 paginiDistinguishing Dementia with Lewy Bodies and Alzheimer's Disease Using MRI and SPECTGabriela MacíasÎncă nu există evaluări
- The Epidemiology and Mutation Types of Leber's Hereditary Optic Neuropathy in ThailandDocument7 paginiThe Epidemiology and Mutation Types of Leber's Hereditary Optic Neuropathy in ThailandKanchy Kanchalika SathianvichitrÎncă nu există evaluări
- Artigo Relacionado Ao NeurodegeneraçãoDocument12 paginiArtigo Relacionado Ao NeurodegeneraçãoJean CarlosÎncă nu există evaluări
- Kwong 2012Document8 paginiKwong 2012Ke XuÎncă nu există evaluări
- Pi Is 0006322317316712Document13 paginiPi Is 0006322317316712Mario JosueÎncă nu există evaluări
- Beyza Ciftci-Kavaklioglu, E Ann Yeh - Ozanimod in Multiple SclerosisDocument11 paginiBeyza Ciftci-Kavaklioglu, E Ann Yeh - Ozanimod in Multiple SclerosisMarina ShinkoÎncă nu există evaluări
- FDG-PET Improves Accuracy in Distinguishing Frontotemporal Dementia and Alzheimer's DiseaseDocument20 paginiFDG-PET Improves Accuracy in Distinguishing Frontotemporal Dementia and Alzheimer's DiseaseMoch Syafrudin RidwanÎncă nu există evaluări
- Sethi 1999Document7 paginiSethi 1999kwpang1Încă nu există evaluări
- DeWire 2022Document14 paginiDeWire 2022docadax848Încă nu există evaluări
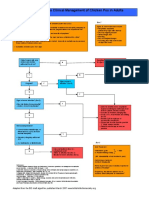
- Chicken Pox Guidelines PDFDocument1 paginăChicken Pox Guidelines PDFAuliaRahmanÎncă nu există evaluări
- Syarah Hikam 1Document108 paginiSyarah Hikam 1AuliaRahmanÎncă nu există evaluări
- Post-Cardiac Arrest SyndromeDocument30 paginiPost-Cardiac Arrest SyndromeAuliaRahmanÎncă nu există evaluări
- Centor ScoreDocument8 paginiCentor ScoreLoo DonÎncă nu există evaluări
- NEWSDocument183 paginiNEWSSebastian BaqueroÎncă nu există evaluări
- RHDDocument130 paginiRHDDeepu RajendranÎncă nu există evaluări
- Anamnesis:: BB KG TB CM No - RM TGL - Masuk TGL - Lahir DPJPDocument4 paginiAnamnesis:: BB KG TB CM No - RM TGL - Masuk TGL - Lahir DPJPAuliaRahmanÎncă nu există evaluări
- Anamnesis:: BB KG TB CM No - RM TGL - Masuk TGL - Lahir DPJPDocument4 paginiAnamnesis:: BB KG TB CM No - RM TGL - Masuk TGL - Lahir DPJPAuliaRahmanÎncă nu există evaluări
- Centor ScoreDocument8 paginiCentor ScoreLoo DonÎncă nu există evaluări
- VACTERL-association EN PDFDocument12 paginiVACTERL-association EN PDFAuliaRahmanÎncă nu există evaluări
- Jurnal OkeDocument8 paginiJurnal OkeAuliaRahmanÎncă nu există evaluări
- Interesting Case March, 15 2016: Sri Yati, Charles, Aulia, Fanny, SasaDocument31 paginiInteresting Case March, 15 2016: Sri Yati, Charles, Aulia, Fanny, SasaAuliaRahmanÎncă nu există evaluări
- 2006 118 1774 Subcommittee On Diagnosis and Management of BronchiolitisDocument22 pagini2006 118 1774 Subcommittee On Diagnosis and Management of BronchiolitisAuliaRahmanÎncă nu există evaluări
- Who TRS 923 PDFDocument130 paginiWho TRS 923 PDFAuliaRahmanÎncă nu există evaluări
- Chicken Pox Guidelines PDFDocument1 paginăChicken Pox Guidelines PDFAuliaRahmanÎncă nu există evaluări
- Igra Factsheet Oct2011 PDFDocument2 paginiIgra Factsheet Oct2011 PDFAuliaRahmanÎncă nu există evaluări
- bRAIN gYMDocument11 paginibRAIN gYMshannay201050% (2)
- Interesting Case March, 15 2016: Sri Yati, Charles, Aulia, Fanny, SasaDocument31 paginiInteresting Case March, 15 2016: Sri Yati, Charles, Aulia, Fanny, SasaAuliaRahmanÎncă nu există evaluări
- Makalah Brain GYM International, BDocument17 paginiMakalah Brain GYM International, BAuliaRahmanÎncă nu există evaluări
- Breastfeeding: Best For Baby and MotherDocument12 paginiBreastfeeding: Best For Baby and MotherSari Whardani Mahligai PateryÎncă nu există evaluări
- Igra Factsheet Oct2011Document2 paginiIgra Factsheet Oct2011AuliaRahmanÎncă nu există evaluări
- Incase Qobam Lab 17 MaretDocument6 paginiIncase Qobam Lab 17 MaretAuliaRahmanÎncă nu există evaluări
- Diagnosis of Childhood Acute Lymphoblastic Leukemia and Optimization of Risk-Benefit Ratio of TherapyDocument24 paginiDiagnosis of Childhood Acute Lymphoblastic Leukemia and Optimization of Risk-Benefit Ratio of TherapyAuliaRahmanÎncă nu există evaluări
- Diagnosis of Childhood Acute Lymphoblastic Leukemia and Optimization of Risk-Benefit Ratio of TherapyDocument24 paginiDiagnosis of Childhood Acute Lymphoblastic Leukemia and Optimization of Risk-Benefit Ratio of TherapyAuliaRahmanÎncă nu există evaluări
- Wilayah 3'-DiterjemahkanDocument1 paginăWilayah 3'-DiterjemahkanAuliaRahmanÎncă nu există evaluări
- Varicella Vaccination AlgorithmDocument1 paginăVaricella Vaccination AlgorithmAuliaRahmanÎncă nu există evaluări
- Interesting Case 27.03.2013Document10 paginiInteresting Case 27.03.2013AuliaRahmanÎncă nu există evaluări
- Interesting Case: Masruri, Esha, Alex, Milza, Wicak, Gita, Zaki, Arin, Eni, FiaDocument10 paginiInteresting Case: Masruri, Esha, Alex, Milza, Wicak, Gita, Zaki, Arin, Eni, FiaAuliaRahmanÎncă nu există evaluări
- Pediatric Dental CareDocument27 paginiPediatric Dental CareAuliaRahmanÎncă nu există evaluări
- How To Install Windows XP From Pen Drive Step by Step GuideDocument3 paginiHow To Install Windows XP From Pen Drive Step by Step GuideJithendra Kumar MÎncă nu există evaluări
- Preparatory Lights and Perfections: Joseph Smith's Training with the Urim and ThummimDocument9 paginiPreparatory Lights and Perfections: Joseph Smith's Training with the Urim and ThummimslightlyguiltyÎncă nu există evaluări
- List of PEGA Interview Questions and AnswersDocument33 paginiList of PEGA Interview Questions and Answersknagender100% (1)
- Digital MarketingDocument70 paginiDigital MarketingTarun N. O'Brain Gahlot0% (2)
- Gujarat Technological University: Emester ViDocument4 paginiGujarat Technological University: Emester ViPradeep SutharÎncă nu există evaluări
- PS Neo HSK2LCD ICON LED RF Keypad v1 0 Installation Guide R001 en FR Es PoDocument40 paginiPS Neo HSK2LCD ICON LED RF Keypad v1 0 Installation Guide R001 en FR Es Po7seguridadÎncă nu există evaluări
- Reasons Why Coca Cola Has A Large Market Share in Kenya and The WorldDocument9 paginiReasons Why Coca Cola Has A Large Market Share in Kenya and The WorldAludahÎncă nu există evaluări
- Surface Coating ProcessesDocument7 paginiSurface Coating ProcessesSailabala ChoudhuryÎncă nu există evaluări
- Judges - God's War Against HumanismDocument347 paginiJudges - God's War Against HumanismgypsylanternÎncă nu există evaluări
- Detailed Lesson Plan in MAPEH III I. ObjectivesDocument19 paginiDetailed Lesson Plan in MAPEH III I. ObjectivesJenna FriasÎncă nu există evaluări
- TelanganaDocument16 paginiTelanganaRamu Palvai0% (1)
- Loverpreet Chapterv 1Document16 paginiLoverpreet Chapterv 1Sheikh SiddiquiÎncă nu există evaluări
- Examples of IELTS Speaking Part 1 QuestionsDocument15 paginiExamples of IELTS Speaking Part 1 QuestionsThanh TrầnÎncă nu există evaluări
- 1651 EE-ES-2019-1015-R0 Load Flow PQ Capability (ENG)Document62 pagini1651 EE-ES-2019-1015-R0 Load Flow PQ Capability (ENG)Alfonso GonzálezÎncă nu există evaluări
- GuideDocument2 paginiGuideMaissyÎncă nu există evaluări
- Technology & Livelihood Education: WEEK 6-7Document28 paginiTechnology & Livelihood Education: WEEK 6-7my musicÎncă nu există evaluări
- AD 251 - Equivalent Uniform Moment Factor, M (Italic)Document1 paginăAD 251 - Equivalent Uniform Moment Factor, M (Italic)symon ellimacÎncă nu există evaluări
- Disappearance of Madeleine McCannDocument36 paginiDisappearance of Madeleine McCannCopernicÎncă nu există evaluări
- Economics and The Theory of Games - Vega-Redondo PDFDocument526 paginiEconomics and The Theory of Games - Vega-Redondo PDFJaime Andrés67% (3)
- Matrices Class 12 Maths Important Questions Chapter 3 - Learn CBSEDocument41 paginiMatrices Class 12 Maths Important Questions Chapter 3 - Learn CBSEkhateeb ul islam qadriÎncă nu există evaluări
- Teaching Support Untuk Managemen HRDocument102 paginiTeaching Support Untuk Managemen HRFernando FmchpÎncă nu există evaluări
- OS9000 AOS 6.1.5 R01 Network Configuration GuideDocument846 paginiOS9000 AOS 6.1.5 R01 Network Configuration GuideclaupasinaÎncă nu există evaluări
- CE ProblemDocument5 paginiCE ProblemJho FÎncă nu există evaluări
- Manual EDocument12 paginiManual EKrum KashavarovÎncă nu există evaluări
- S4 - SD - HOTS in Practice - EnglishDocument65 paginiS4 - SD - HOTS in Practice - EnglishIries DanoÎncă nu există evaluări
- E.sybox - Esybox All Information PDFDocument56 paginiE.sybox - Esybox All Information PDFnle_16948Încă nu există evaluări
- Surface water drainage infiltration testingDocument8 paginiSurface water drainage infiltration testingRay CooperÎncă nu există evaluări
- Automotive E-Coat Paint Process Simulation Using FEADocument20 paginiAutomotive E-Coat Paint Process Simulation Using FEAflowh_100% (1)
- Arts9 q4 Mod1 Theatricalforms v5Document30 paginiArts9 q4 Mod1 Theatricalforms v5Harold RicafortÎncă nu există evaluări
- XYZ Company Asset Inventory ReportDocument1 paginăXYZ Company Asset Inventory ReportNini KitsÎncă nu există evaluări