S-ar putea să vă placă și
- Cakupan Imunisasi Tahun 2018Document2 paginiCakupan Imunisasi Tahun 2018juita auglinaÎncă nu există evaluări
- Nursing Management-Module II-LearnersDocument83 paginiNursing Management-Module II-Learnersjuita auglinaÎncă nu există evaluări
- Malaria With Hyperbilirubinemia in MinahasaDocument14 paginiMalaria With Hyperbilirubinemia in Minahasajuita auglinaÎncă nu există evaluări
- List Pasien Divisi Digestive 27 JUNI 2013: Irina A AtasDocument6 paginiList Pasien Divisi Digestive 27 JUNI 2013: Irina A Atasjuita auglinaÎncă nu există evaluări
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (345)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Clinical Pathology: Essentials ofDocument8 paginiClinical Pathology: Essentials ofAhmed BahaaÎncă nu există evaluări
- Medical Practitioner Curriculum VitaeDocument2 paginiMedical Practitioner Curriculum VitaesamiÎncă nu există evaluări
- T Dr. Gharama Al-Shehri: Asir Surgical Residency ProgramDocument3 paginiT Dr. Gharama Al-Shehri: Asir Surgical Residency ProgramKhaled Shaheen100% (1)
- History and Evolution of TelemedicineDocument2 paginiHistory and Evolution of TelemedicineKamila HiÎncă nu există evaluări
- Cancer NotesDocument1 paginăCancer NotesJery KavilpuraidomÎncă nu există evaluări
- Ornap 2012Document2 paginiOrnap 2012Harby Ongbay AbellanosaÎncă nu există evaluări
- HalmaDocument16 paginiHalmanishanthpv3Încă nu există evaluări
- SJT Answers & RationaleDocument76 paginiSJT Answers & RationaleFarhan SakunÎncă nu există evaluări
- The Art of PhacoemulsificationDocument544 paginiThe Art of PhacoemulsificationDaniel Fernández Gajardo100% (3)
- Notification Dr. Baba Saheb Ambedkar Hospital Senior Resident PostsDocument5 paginiNotification Dr. Baba Saheb Ambedkar Hospital Senior Resident PostsJeshiÎncă nu există evaluări
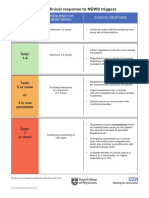
- Outline Clinical Response To News Triggers (With Explanatory Text) - 0 - 0 - 0Document2 paginiOutline Clinical Response To News Triggers (With Explanatory Text) - 0 - 0 - 0John SmithyÎncă nu există evaluări
- PRCDocument6 paginiPRCKate ChavezÎncă nu există evaluări
- Medical Services Recruitment Board (MRB) : Notification No. 4/MRB/E4/2013 Dated: 12.06.2013Document5 paginiMedical Services Recruitment Board (MRB) : Notification No. 4/MRB/E4/2013 Dated: 12.06.2013kumarÎncă nu există evaluări
- CV RobbyDocument3 paginiCV RobbygerryÎncă nu există evaluări
- Eizenberg's General AnatomyDocument255 paginiEizenberg's General Anatomymushroom620100% (9)
- Definitions of SurgeryDocument6 paginiDefinitions of SurgeryPrince SyahirÎncă nu există evaluări
- MDI2conforme2017 18Document1 paginăMDI2conforme2017 18Apryl Phyllis JimenezÎncă nu există evaluări
- WRBFS407BDocument100 paginiWRBFS407BIon Logofătu AlbertÎncă nu există evaluări
- Episiotomy PDFDocument54 paginiEpisiotomy PDFputri diana100% (1)
- Scott Devlin Resume 2Document2 paginiScott Devlin Resume 2api-355272879Încă nu există evaluări
- Doctors ListDocument10 paginiDoctors ListsureshÎncă nu există evaluări
- Advertisement Grade A CAS MaharastraDocument5 paginiAdvertisement Grade A CAS MaharastraDrRam Jadhav LakavathÎncă nu există evaluări
- Biology - Knee Jerk SPMDocument4 paginiBiology - Knee Jerk SPMKumar AyavooÎncă nu există evaluări
- Operating Room Requirements For 2014 and Beyond: 2014 FGI Guidelines Update SeriesDocument6 paginiOperating Room Requirements For 2014 and Beyond: 2014 FGI Guidelines Update Series0307aliÎncă nu există evaluări
- Mechanisms of CarcinogenESIS PDFDocument37 paginiMechanisms of CarcinogenESIS PDFJessenia ZuritaÎncă nu există evaluări
- Alyssa Mellott ResumeDocument2 paginiAlyssa Mellott Resumeapi-281921437Încă nu există evaluări
- 1609cei Ellenbogen WebDocument8 pagini1609cei Ellenbogen WebAbhishek Isaac MathewÎncă nu există evaluări
- Necrotising Enterocolitis in Infants On NICU JCG0038 v2Document11 paginiNecrotising Enterocolitis in Infants On NICU JCG0038 v2RatnaArdianaNoviantiÎncă nu există evaluări
- StratOG Vaginal BreechDocument17 paginiStratOG Vaginal BreechNalin AbeysingheÎncă nu există evaluări
- Bombay Hospital InformationBookletDocument12 paginiBombay Hospital InformationBookletmilkywayÎncă nu există evaluări