S-ar putea să vă placă și
- Recipe Booklet PRINT VERSIONDocument40 paginiRecipe Booklet PRINT VERSIONjtsunami815100% (1)
- LR 1350 Operating InstructionsDocument1.495 paginiLR 1350 Operating InstructionsPatrick Polujan100% (12)
- AG C O L: Uide To Ommon RAL EsionsDocument46 paginiAG C O L: Uide To Ommon RAL EsionsAndykaYayanSetiawanÎncă nu există evaluări
- AG C O L: Uide To Ommon RAL EsionsDocument46 paginiAG C O L: Uide To Ommon RAL EsionsAndykaYayanSetiawanÎncă nu există evaluări
- AG C O L: Uide To Ommon RAL EsionsDocument46 paginiAG C O L: Uide To Ommon RAL EsionsAndykaYayanSetiawanÎncă nu există evaluări
- Tongue Lession PrintDocument9 paginiTongue Lession Printdlami_ahÎncă nu există evaluări
- Textbook of Oral Medicine PDFDocument1.179 paginiTextbook of Oral Medicine PDFwenny100% (1)
- Manual Jib 25 10 02Document256 paginiManual Jib 25 10 02Luis Jose LlobanÎncă nu există evaluări
- 3 Composites PDFDocument14 pagini3 Composites PDFKavya ulliÎncă nu există evaluări
- Heat Shrink CoatingDocument5 paginiHeat Shrink CoatingMekhmanÎncă nu există evaluări
- Geographic TongueDocument5 paginiGeographic Tonguebhawna_aroraÎncă nu există evaluări
- Oral Pathology - Clinical Pathologic Correlations - 6th - EdDocument4 paginiOral Pathology - Clinical Pathologic Correlations - 6th - EdwennyÎncă nu există evaluări
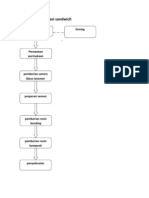
- Prosedur Restorasi SandwichDocument6 paginiProsedur Restorasi SandwichMaria Apriliana100% (1)
- Manual L W26Document436 paginiManual L W26Taufan ArifÎncă nu există evaluări
- Geographic Tongue: Clinical Characteristics of 188 CasesDocument11 paginiGeographic Tongue: Clinical Characteristics of 188 CasesMahendra PrihandanaÎncă nu există evaluări
- Benign Migratory Glossitis: A Review: KeywordsDocument11 paginiBenign Migratory Glossitis: A Review: KeywordsDita Merry Diah VanonyÎncă nu există evaluări
- Geographic Tongue and Psoriasis: Clinical, Histopathological, Immunohistochemical and Genetic Correlation - A Literature ReviewDocument12 paginiGeographic Tongue and Psoriasis: Clinical, Histopathological, Immunohistochemical and Genetic Correlation - A Literature ReviewwennyÎncă nu există evaluări
- Geographic Tongue in Monozygotic Twins: Abst TDocument2 paginiGeographic Tongue in Monozygotic Twins: Abst Twafiqah izzatul auliahÎncă nu există evaluări
- Geographic Tongue Literature Review and Case ReportsDocument5 paginiGeographic Tongue Literature Review and Case ReportsafmznqfsclmgbeÎncă nu există evaluări
- Paediatric Geographic Tongue: A Case Report, Review and Recent UpdatesDocument5 paginiPaediatric Geographic Tongue: A Case Report, Review and Recent UpdatespipitÎncă nu există evaluări
- Glositis Dan AtopiDocument6 paginiGlositis Dan AtopiAmanda Rizka PutriÎncă nu există evaluări
- Benign Migratory Glossitis and AllergyDocument2 paginiBenign Migratory Glossitis and AllergyAfifah Novita YuliastutiÎncă nu există evaluări
- The Relationship Between Geographic Tongue and Stress: H Ebrahimi, S Pourshahidi, A Andisheh Tadbir, S Bakhshi ShyanDocument3 paginiThe Relationship Between Geographic Tongue and Stress: H Ebrahimi, S Pourshahidi, A Andisheh Tadbir, S Bakhshi ShyanCikw KuzhaÎncă nu există evaluări
- Dental JOURNAL: Geographic Tongue in A 6 Year Old Child: A Case Report With Review of LiteratureDocument6 paginiDental JOURNAL: Geographic Tongue in A 6 Year Old Child: A Case Report With Review of LiteraturewennyÎncă nu există evaluări
- Riga-Fede Traumatic LingualDocument5 paginiRiga-Fede Traumatic LingualrlagistaÎncă nu există evaluări
- 3 Case Report Geographic Tongue Haritsa BudimanDocument10 pagini3 Case Report Geographic Tongue Haritsa Budimanharitsa budimanÎncă nu există evaluări
- Geographic Tongue 2Document8 paginiGeographic Tongue 2ahya azizahÎncă nu există evaluări
- Distribution of Geographic Tongue On Dentistry Student Gadjah Mada University of YogyakartaDocument7 paginiDistribution of Geographic Tongue On Dentistry Student Gadjah Mada University of YogyakartaKhusnul SyamsuddinÎncă nu există evaluări
- Burning Mouth Syndrome: A Case ReportDocument3 paginiBurning Mouth Syndrome: A Case ReportRina KartikaÎncă nu există evaluări
- Gene/environment Causes of Cleft Lip And/or Palate: Developmental Biology: Frontiers For Clinical GeneticsDocument9 paginiGene/environment Causes of Cleft Lip And/or Palate: Developmental Biology: Frontiers For Clinical GeneticsGrazyele SantanaÎncă nu există evaluări
- Systematic Review: Geographical and Ethnic Differences in Gastro-Oesophageal Reflux DiseaseDocument13 paginiSystematic Review: Geographical and Ethnic Differences in Gastro-Oesophageal Reflux DiseaseArum Sekarwage J RÎncă nu există evaluări
- 3.tahrir N. Aldelaimi Article Occurrence of Lichen Planus in Diabetes MellitusDocument4 pagini3.tahrir N. Aldelaimi Article Occurrence of Lichen Planus in Diabetes MellitusMohammed AbdulhammedÎncă nu există evaluări
- Geographic Tongue in Psoriasis Case ReportsDocument5 paginiGeographic Tongue in Psoriasis Case Reportsanindita mayaÎncă nu există evaluări
- Geographic Tongue IsDocument2 paginiGeographic Tongue IsNa DiaÎncă nu există evaluări
- Pod PDFDocument3 paginiPod PDFTri Pamungkas IrawanÎncă nu există evaluări
- Oral Lesions in Leprosy Revisited: A Case Report: A. K. Dhawan, MD, Prashant Verma, MD, and S. Sharma, MDDocument2 paginiOral Lesions in Leprosy Revisited: A Case Report: A. K. Dhawan, MD, Prashant Verma, MD, and S. Sharma, MDOjanÎncă nu există evaluări
- 2003, Vol.21, Issues 1, Oral Medicine and Oral DermatologyDocument212 pagini2003, Vol.21, Issues 1, Oral Medicine and Oral DermatologyRizweta DestinÎncă nu există evaluări
- Microbiota LinguaDocument15 paginiMicrobiota LinguaIlana FuxÎncă nu există evaluări
- Occurrence of Recurrent Aphthous Stomatitis (RAS) As A Rare Oral Manifestation in A Patient With Gilbert's SyndromeDocument5 paginiOccurrence of Recurrent Aphthous Stomatitis (RAS) As A Rare Oral Manifestation in A Patient With Gilbert's SyndromeDinesh RokayaÎncă nu există evaluări
- Burning Mouth Syndrome An Update 2010Document7 paginiBurning Mouth Syndrome An Update 2010tele6Încă nu există evaluări
- Benign Migratory Glossitis: Case Report and Literature ReviewDocument3 paginiBenign Migratory Glossitis: Case Report and Literature ReviewBharat NarumanchiÎncă nu există evaluări
- Case Report: Idiopathic Orofacial Granulomatosis With Varied Clinical PresentationDocument4 paginiCase Report: Idiopathic Orofacial Granulomatosis With Varied Clinical PresentationPrince AhmedÎncă nu există evaluări
- Cibirka1997 BMS Classic ArticleDocument5 paginiCibirka1997 BMS Classic ArticleDr FarhatÎncă nu există evaluări
- Childhood Lichen Planus With Palmoplantar InvolvementDocument3 paginiChildhood Lichen Planus With Palmoplantar InvolvementSabriadi NursalÎncă nu există evaluări
- BrazJOralSci 2011 Vol10 Issue4 p288 93Document6 paginiBrazJOralSci 2011 Vol10 Issue4 p288 93Tri Sakti Sunda RomdhoniÎncă nu există evaluări
- Fissured Tongue: A Case Report and Review of Literature: KeywordsDocument5 paginiFissured Tongue: A Case Report and Review of Literature: Keywordssiti baiq gadishaÎncă nu există evaluări
- Geographic Tongue Severity Index A New and Clinical Scoring SystemDocument9 paginiGeographic Tongue Severity Index A New and Clinical Scoring SystemNurlina NurdinÎncă nu există evaluări
- Oral Lichen Planus Clinical Features, Etiology, Treatment andDocument7 paginiOral Lichen Planus Clinical Features, Etiology, Treatment andevhafadlianurÎncă nu există evaluări
- Oral Manifestations of Systemic Disease: Autoimmune DiseasesDocument7 paginiOral Manifestations of Systemic Disease: Autoimmune DiseaseshussainÎncă nu există evaluări
- Laryngomalacia and Swallowing Function in ChildrenDocument7 paginiLaryngomalacia and Swallowing Function in ChildrenmelaniaÎncă nu există evaluări
- (Louis Et Al., 1987) Candidal Infection of The Tongue With Nonspecific Inflammation of The PalateDocument5 pagini(Louis Et Al., 1987) Candidal Infection of The Tongue With Nonspecific Inflammation of The PalateAFINA MUTIAH TUHEPALYÎncă nu există evaluări
- Multiple Bilateral Taurodontism. A Case ReportDocument3 paginiMultiple Bilateral Taurodontism. A Case ReportJing XueÎncă nu există evaluări
- Pyogenic Granuloma - A Clinicopathological Analysis of Fifty Cases - Ujwala Rohan Newadkar, Swapnil Khairnar, Arun Dodamani, Journal of Oral Research and ReviewDocument4 paginiPyogenic Granuloma - A Clinicopathological Analysis of Fifty Cases - Ujwala Rohan Newadkar, Swapnil Khairnar, Arun Dodamani, Journal of Oral Research and ReviewfaridaÎncă nu există evaluări
- Symptomatic BenignDocument5 paginiSymptomatic BenignTri Pamungkas IrawanÎncă nu există evaluări
- Piis0736467917308922 PDFDocument2 paginiPiis0736467917308922 PDFNenny HariyantoÎncă nu există evaluări
- White Sponge NevusDocument2 paginiWhite Sponge Nevusbundahara zoomÎncă nu există evaluări
- TODENTJ 10 619 CompressedDocument17 paginiTODENTJ 10 619 CompressedAisyah Arina NurhafizahÎncă nu există evaluări
- Bahan DressingDocument17 paginiBahan DressingRinanda YuliaÎncă nu există evaluări
- Childhood Oral Lichen Planus: Report of Two CasesDocument5 paginiChildhood Oral Lichen Planus: Report of Two CasesFuad HasanÎncă nu există evaluări
- 14 1 Association Interleukin BayoumiDocument8 pagini14 1 Association Interleukin BayoumiNadya PurwantyÎncă nu există evaluări
- Walsh 2019Document17 paginiWalsh 2019madhumitha srinivasÎncă nu există evaluări
- Oral Findings of Systemic Lupus Erythematosus - A Grand Round CaseDocument6 paginiOral Findings of Systemic Lupus Erythematosus - A Grand Round CaseArditya Dwi YudistiraÎncă nu există evaluări
- Medoralv16 I6 p745 PDFDocument5 paginiMedoralv16 I6 p745 PDFAyu Ervita HydayatyÎncă nu există evaluări
- Fissured Tongue: A Case Report and Review of Literature: KeywordsDocument5 paginiFissured Tongue: A Case Report and Review of Literature: Keywordspink_grcq_sssttt4836Încă nu există evaluări
- Jurnal 2Document11 paginiJurnal 2M Addien Prima NandaÎncă nu există evaluări
- Down SyndromeDocument3 paginiDown SyndromeIdelia GunawanÎncă nu există evaluări
- Is Caviar Disease (Sublingual Varices) Associated With Trauma?Document2 paginiIs Caviar Disease (Sublingual Varices) Associated With Trauma?Mardiyah PratiwiÎncă nu există evaluări
- Lack of Association Between Celiac Disease and Dental Enamel HypoplasiaDocument6 paginiLack of Association Between Celiac Disease and Dental Enamel HypoplasiaLjubomirErdoglijaÎncă nu există evaluări
- Halitosis: An Overview of Epidemiology, Etiology and Clinical ManagementDocument6 paginiHalitosis: An Overview of Epidemiology, Etiology and Clinical Managementdrmezzo68Încă nu există evaluări
- 565 FullDocument2 pagini565 FullTrikala2016Încă nu există evaluări
- Laryngopharyngeal and Gastroesophageal Reflux: A Comprehensive Guide to Diagnosis, Treatment, and Diet-Based ApproachesDe la EverandLaryngopharyngeal and Gastroesophageal Reflux: A Comprehensive Guide to Diagnosis, Treatment, and Diet-Based ApproachesCraig H. ZalvanÎncă nu există evaluări
- Produce101s2 PDFDocument22 paginiProduce101s2 PDFwennyÎncă nu există evaluări
- Sist. Urine 2015 2Document37 paginiSist. Urine 2015 2wennyÎncă nu există evaluări
- Podj 3 PDFDocument2 paginiPodj 3 PDFwennyÎncă nu există evaluări
- Handbook of Oral Diseases 1 Edition PDFDocument30 paginiHandbook of Oral Diseases 1 Edition PDFwennyÎncă nu există evaluări
- Geographic TongueDocument2 paginiGeographic TonguewennyÎncă nu există evaluări
- GypsumDocument14 paginiGypsummuskanÎncă nu există evaluări
- GypsumDocument14 paginiGypsummuskanÎncă nu există evaluări
- 4Document5 pagini4wennyÎncă nu există evaluări
- Dental JOURNAL: Geographic Tongue in A 6 Year Old Child: A Case Report With Review of LiteratureDocument6 paginiDental JOURNAL: Geographic Tongue in A 6 Year Old Child: A Case Report With Review of LiteraturewennyÎncă nu există evaluări
- 4Document5 pagini4wennyÎncă nu există evaluări
- Immunology Dental CariesDocument24 paginiImmunology Dental CarieswennyÎncă nu există evaluări
- Eaton BECOPAD P Range TechnicalDataSheet enDocument4 paginiEaton BECOPAD P Range TechnicalDataSheet enEsteban Fernando Meza IbacetaÎncă nu există evaluări
- Lem Cyclop Ewt Owner S Manual 10Document10 paginiLem Cyclop Ewt Owner S Manual 10josep_garcía_16Încă nu există evaluări
- NOTIFIER ERCES-Bi-Directional Amplifier Systems (BDA) Webinar 6-4-2019Document50 paginiNOTIFIER ERCES-Bi-Directional Amplifier Systems (BDA) Webinar 6-4-2019culeros1Încă nu există evaluări
- Neurology and Special Senses: High-Yield SystemsDocument72 paginiNeurology and Special Senses: High-Yield SystemsMahmoud Abu MayalehÎncă nu există evaluări
- Calamity and Disaster Preparedness Chapter IXDocument34 paginiCalamity and Disaster Preparedness Chapter IXANGEL ALBERTÎncă nu există evaluări
- MS Fresher HR DocumentDocument4 paginiMS Fresher HR DocumentJahanvi KambojÎncă nu există evaluări
- 06-433rev7 HFC-227ea IVO ManualDocument109 pagini06-433rev7 HFC-227ea IVO ManualFelix MartinezÎncă nu există evaluări
- Normal Microflora of Human BodyDocument14 paginiNormal Microflora of Human BodySarah PavuÎncă nu există evaluări
- New-DLP Phase2 Assignment-3 Module-B Final-9.8.18Document6 paginiNew-DLP Phase2 Assignment-3 Module-B Final-9.8.18PÎncă nu există evaluări
- Topic 10 - The Schooler and The FamilyDocument18 paginiTopic 10 - The Schooler and The FamilyReanne Mae AbreraÎncă nu există evaluări
- iGCSE Biology Section 1 Lesson 1Document44 paginiiGCSE Biology Section 1 Lesson 1aastha dograÎncă nu există evaluări
- q5 Nursery SchoolDocument4 paginiq5 Nursery SchoolPK CheahÎncă nu există evaluări
- Compositional Changes of Crude Oil SARA Fractions Due To Biodegradation and Adsorption Supported On Colloidal Support Such As Clay Susing IatroscanDocument13 paginiCompositional Changes of Crude Oil SARA Fractions Due To Biodegradation and Adsorption Supported On Colloidal Support Such As Clay Susing IatroscanNatalia KovalovaÎncă nu există evaluări
- Performantele MTADocument5 paginiPerformantele MTAana aÎncă nu există evaluări
- FCE Writing 14 - ArticleDocument4 paginiFCE Writing 14 - Articlepingu70Încă nu există evaluări
- Solid Dosage Form Part 1Document48 paginiSolid Dosage Form Part 1Claire Marie AlvaranÎncă nu există evaluări
- Rodents and Sectional Title ComplexDocument2 paginiRodents and Sectional Title ComplexFredSmith777Încă nu există evaluări
- HRM Report CIA 3Document5 paginiHRM Report CIA 3SUNIDHI PUNDHIR 20221029Încă nu există evaluări
- Breastfeeding PlanDocument7 paginiBreastfeeding Planapi-223713414Încă nu există evaluări
- Ragin Cajun PDFDocument2 paginiRagin Cajun PDFjosemfcÎncă nu există evaluări
- 8DJ - 8DH Katalog en PDFDocument32 pagini8DJ - 8DH Katalog en PDFJosue Espinoza YachachinÎncă nu există evaluări
- Medical Gases: NO. Item Brand Name OriginDocument4 paginiMedical Gases: NO. Item Brand Name OriginMahmoud AnwerÎncă nu există evaluări
- Types of Business OwnershipDocument2 paginiTypes of Business Ownershipprelovedseller bnÎncă nu există evaluări
- Teoria Do Campo Ligante - Part IIDocument25 paginiTeoria Do Campo Ligante - Part IIArthurGrafdeSousaÎncă nu există evaluări