S-ar putea să vă placă și
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (399)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- MCMI-IV Interpretive Report - 6856501 - 20180509033028436 PDFDocument10 paginiMCMI-IV Interpretive Report - 6856501 - 20180509033028436 PDFChristianJ.Rodriguez100% (1)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (73)
- A HOFFER Review Niacin The Real StoryDocument2 paginiA HOFFER Review Niacin The Real StoryAna Lu100% (1)
- Acquired Brain en Una Tienda de LibrosDocument428 paginiAcquired Brain en Una Tienda de Libroslig100% (1)
- Bi PAPDocument30 paginiBi PAPraerlnÎncă nu există evaluări
- MED 2 Electrical Safety Test of Medical Equipment After RepairDocument17 paginiMED 2 Electrical Safety Test of Medical Equipment After RepairAfiz86Încă nu există evaluări
- ObjectivesDocument2 paginiObjectivesAmy RamirezÎncă nu există evaluări
- Application CoopMED Health Insurance Plan BarbadosDocument2 paginiApplication CoopMED Health Insurance Plan BarbadosKammieÎncă nu există evaluări
- SerologyDocument33 paginiSerologyGEBEYAW ADDISUÎncă nu există evaluări
- 03chapter4 PDFDocument72 pagini03chapter4 PDFAnonymous bT8Fs8daY2Încă nu există evaluări
- Counseling Theories Applied to JakeDocument2 paginiCounseling Theories Applied to JakeArielle RamirezÎncă nu există evaluări
- Capstone PosterDocument1 paginăCapstone Posterapi-273438577Încă nu există evaluări
- Oral Cancer BDADocument36 paginiOral Cancer BDAJesús De Santos AlbaÎncă nu există evaluări
- Chron Skin Allergy Oct 2010Document32 paginiChron Skin Allergy Oct 2010shannon3458Încă nu există evaluări
- Cleft Lip or Cleft Palate / Pharyngoplasty Clinical Pathway: Personal DetailsDocument8 paginiCleft Lip or Cleft Palate / Pharyngoplasty Clinical Pathway: Personal DetailsRegine LacosteÎncă nu există evaluări
- E A R D o C 2010 InvDocument16 paginiE A R D o C 2010 InvBarak ShitritÎncă nu există evaluări
- Tool and Resource Evaluation TemplateDocument4 paginiTool and Resource Evaluation Templatetimie_reyesÎncă nu există evaluări
- Third Molar Agenesis and How It Relates To The Modern HygienistDocument17 paginiThird Molar Agenesis and How It Relates To The Modern HygienistAmanda StewartÎncă nu există evaluări
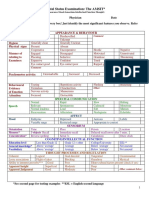
- Mental Status Examination: The AMSIT : Neat and Tidy DisshevelledDocument2 paginiMental Status Examination: The AMSIT : Neat and Tidy Disshevellednisreen100% (1)
- DocumentationDocument11 paginiDocumentationjoyveeÎncă nu există evaluări
- Tugas 2 BHS Ing Rani OctalyaDocument3 paginiTugas 2 BHS Ing Rani OctalyaRozaq Permana YudhaÎncă nu există evaluări
- ORTHOPAEDICS TRAUMADocument33 paginiORTHOPAEDICS TRAUMARhomizal MazaliÎncă nu există evaluări
- Antimicrobial ChemotherapyDocument160 paginiAntimicrobial Chemotherapyokumu atanas0% (1)
- Effects of Maitland Mobilization and Mul PDFDocument6 paginiEffects of Maitland Mobilization and Mul PDFKuroha Hagane KunÎncă nu există evaluări
- Rivotril 0.5mg Tablets Rivotril 2mg TabletsDocument4 paginiRivotril 0.5mg Tablets Rivotril 2mg TabletsМаргарет ВејдÎncă nu există evaluări
- Principles of Hand WashingDocument42 paginiPrinciples of Hand WashingGregorio Crosser100% (1)
- LCD PresentationDocument38 paginiLCD PresentationAnaz HamzaÎncă nu există evaluări
- Clinical AssignmentDocument9 paginiClinical AssignmentkomalÎncă nu există evaluări
- Peads - Diamond Blackfan AnemiaDocument40 paginiPeads - Diamond Blackfan AnemiaBaran PalanimuthuÎncă nu există evaluări
- Management Placenta PreviaDocument24 paginiManagement Placenta PreviaMuhammad RifaldiÎncă nu există evaluări
- Source Information: Disclosure FormsDocument1 paginăSource Information: Disclosure FormsSav GaÎncă nu există evaluări