S-ar putea să vă placă și
- Living and radiological anatomy of the head and neck for dental studentsDe la EverandLiving and radiological anatomy of the head and neck for dental studentsEvaluare: 4 din 5 stele4/5 (1)
- Jaw Relation: DR Gayathri GangadharanDocument65 paginiJaw Relation: DR Gayathri GangadharanGayathri GangadharanÎncă nu există evaluări
- Dental Jurisprudence, Ethics and Practice ManagementDocument9 paginiDental Jurisprudence, Ethics and Practice ManagementFatima CarlosÎncă nu există evaluări
- Optimizing Smile Composition and Esthetics With Resin Composites and Other Conservative Esthetic ProceduresDocument16 paginiOptimizing Smile Composition and Esthetics With Resin Composites and Other Conservative Esthetic ProceduresTiagoÎncă nu există evaluări
- Anat of Root Apex - Review ArticleDocument9 paginiAnat of Root Apex - Review ArticleRevathy ParthasarathyÎncă nu există evaluări
- Occlusal Cant (Autosaved)Document48 paginiOcclusal Cant (Autosaved)Gauri KhadeÎncă nu există evaluări
- Dr.E 2019Document404 paginiDr.E 2019HaifaÎncă nu există evaluări
- Understanding Factors in Uencing Compliance With Removable Functional Appliances: A Qualitative StudyDocument9 paginiUnderstanding Factors in Uencing Compliance With Removable Functional Appliances: A Qualitative StudyMonojit DuttaÎncă nu există evaluări
- EASY QUESTIONS ON PERIODONTICS - Q AsDocument14 paginiEASY QUESTIONS ON PERIODONTICS - Q AsMeena KulkarniÎncă nu există evaluări
- Fronto Facial AnalysisDocument10 paginiFronto Facial AnalysisMariyam100% (1)
- Comparison Between 2D Cephalometric and 3D Digital Model Superimpositions in Patients With Lateral Incisor Agenesis Treated by Canine SubstitutionDocument10 paginiComparison Between 2D Cephalometric and 3D Digital Model Superimpositions in Patients With Lateral Incisor Agenesis Treated by Canine Substitutionhasan.abomohamedÎncă nu există evaluări
- An Assessment of The Relationship Between The Maxillary Sinus Floor and The Maxillary Posterior Teeth Root Tips Using Dental Cone-Beam Computerized TomographyDocument6 paginiAn Assessment of The Relationship Between The Maxillary Sinus Floor and The Maxillary Posterior Teeth Root Tips Using Dental Cone-Beam Computerized TomographyLuciana EspinosaÎncă nu există evaluări
- Asimetria 2d y 3dDocument8 paginiAsimetria 2d y 3dRosa Natalia Muente RojasÎncă nu există evaluări
- Changes in Facial Form Relative To Progressive Atrophy of The Edentulous JawsDocument7 paginiChanges in Facial Form Relative To Progressive Atrophy of The Edentulous JawsshraddhaÎncă nu există evaluări
- S 0039 1697866Document6 paginiS 0039 1697866alejandraÎncă nu există evaluări
- Maxillary Arch Perimeter Prediction Using Ramanujan's Equation For The EllipseDocument7 paginiMaxillary Arch Perimeter Prediction Using Ramanujan's Equation For The Ellipseahmed_awad_36Încă nu există evaluări
- Online Only Abstracts - YmodDocument5 paginiOnline Only Abstracts - YmodDr.Prakher SainiÎncă nu există evaluări
- Comparison Between Skeletal, and Facial Measurements of Vertical Dimension in Edentulous PatientsDocument4 paginiComparison Between Skeletal, and Facial Measurements of Vertical Dimension in Edentulous Patientspaula catanaÎncă nu există evaluări
- ArticulkoDocument4 paginiArticulkoSandy Hernández MalcaÎncă nu există evaluări
- Posterior Crossbite With Mandibular Asymmetry Treated With Lingual Appliances, Maxillary Skeletal Expanders, and Alveolar Bone MiniscrewsDocument21 paginiPosterior Crossbite With Mandibular Asymmetry Treated With Lingual Appliances, Maxillary Skeletal Expanders, and Alveolar Bone MiniscrewsJuliana ÁlvarezÎncă nu există evaluări
- Dentofacial Asymmetries: Challenging Diagnosis and Treatment PlanningDocument4 paginiDentofacial Asymmetries: Challenging Diagnosis and Treatment Planningblogger bloggerÎncă nu există evaluări
- Determining of Canine Position by Multiple Facial Landmark Achieve Natural Esthetics in Complete Denture TreatmentDocument6 paginiDetermining of Canine Position by Multiple Facial Landmark Achieve Natural Esthetics in Complete Denture TreatmentNoviÎncă nu există evaluări
- 1-S2.0-S0278239119305518-MainDocument15 pagini1-S2.0-S0278239119305518-MainALEJANDRA INÉS NIETO ARIASÎncă nu există evaluări
- Surgically Assisted Maxillary Expansion: Norman J. Betts, DDS, MSDocument11 paginiSurgically Assisted Maxillary Expansion: Norman J. Betts, DDS, MSAngélica Valenzuela AndrighiÎncă nu există evaluări
- Biomechanical Considerations For Total Distalization of The Mandibular Dentition in The Treatment of Class III MalocclusionDocument9 paginiBiomechanical Considerations For Total Distalization of The Mandibular Dentition in The Treatment of Class III Malocclusion허성수Încă nu există evaluări
- Arch ExpansionDocument36 paginiArch ExpansionOsama GamilÎncă nu există evaluări
- Kim 2019Document9 paginiKim 2019Dela MedinaÎncă nu există evaluări
- Comparison of Overjet Among 3 Arch Types in Normal OcclusionDocument8 paginiComparison of Overjet Among 3 Arch Types in Normal OcclusionAlexandra308Încă nu există evaluări
- Maxillary Arch Distalization Using Interradicular Miniscrews and The Lever-Arm ApplianceDocument8 paginiMaxillary Arch Distalization Using Interradicular Miniscrews and The Lever-Arm ApplianceJuan Carlos CárcamoÎncă nu există evaluări
- Caninelocalization JNDADocument9 paginiCaninelocalization JNDAshargunan11Încă nu există evaluări
- 3A 2B Immediate ImplantDocument6 pagini3A 2B Immediate ImplantAhmed BadrÎncă nu există evaluări
- Tseng 2016Document12 paginiTseng 2016Amalia Alexandra ZanadÎncă nu există evaluări
- Garrett 2008Document11 paginiGarrett 2008Swadhinata HÎncă nu există evaluări
- Usumi Fujita2018Document15 paginiUsumi Fujita2018Yeimi ArdilaÎncă nu există evaluări
- Miner2012parte 1Document8 paginiMiner2012parte 1bricevargas023Încă nu există evaluări
- Asimetrii MandibulareDocument25 paginiAsimetrii MandibulareBranici OanaÎncă nu există evaluări
- Gallone 2019Document11 paginiGallone 2019MihaiÎncă nu există evaluări
- Comparison of Different Midsagittal Plane Conf 2017 American Journal of OrthDocument10 paginiComparison of Different Midsagittal Plane Conf 2017 American Journal of Orthdruzair007Încă nu există evaluări
- 6 Asimetria MandibularDocument7 pagini6 Asimetria Mandibularmauricia ester caceres candiaÎncă nu există evaluări
- Three-Dimensional Evaluation of Dentofacial Transverse Widths in Adults With Different Sagittal Facial Patterns PDFDocument10 paginiThree-Dimensional Evaluation of Dentofacial Transverse Widths in Adults With Different Sagittal Facial Patterns PDFSoe San KyawÎncă nu există evaluări
- Ne 2Document7 paginiNe 2Zaid DewachiÎncă nu există evaluări
- Podesser 2004Document7 paginiPodesser 2004Tien Li AnÎncă nu există evaluări
- International Journal of Pediatric Otorhinolaryngology: SciencedirectDocument5 paginiInternational Journal of Pediatric Otorhinolaryngology: SciencedirectDiego Andres Hincapie HerreraÎncă nu există evaluări
- Cephalometric TracingDocument10 paginiCephalometric TracingMhmd AbdellatifÎncă nu există evaluări
- EtiologiaDocument9 paginiEtiologiaAriana AmarilesÎncă nu există evaluări
- AJODO Correa 2013Document9 paginiAJODO Correa 2013Samantha OrtizÎncă nu există evaluări
- Articulo 10Document10 paginiArticulo 10Daniela NarváezÎncă nu există evaluări
- New Space Analysis 2021-2022Document23 paginiNew Space Analysis 2021-2022AseelÎncă nu există evaluări
- Space AnalysisDocument8 paginiSpace AnalysisMohammed JaberÎncă nu există evaluări
- On The Interaction Between Incisor Crown-Root Morphology and Third-Order AngulationDocument8 paginiOn The Interaction Between Incisor Crown-Root Morphology and Third-Order Angulationali.celik1347Încă nu există evaluări
- Vertical Jaw Relation: V.S.HarishDocument17 paginiVertical Jaw Relation: V.S.HarishHarish VsÎncă nu există evaluări
- Kim 2023Document11 paginiKim 2023Dela MedinaÎncă nu există evaluări
- Orthodontic Correction of Anterior Crossbite in An Adult PatientDocument5 paginiOrthodontic Correction of Anterior Crossbite in An Adult PatientGoutamÎncă nu există evaluări
- Smile Dent J 2012 7 1 44 49Document6 paginiSmile Dent J 2012 7 1 44 49MQ SpotifyÎncă nu există evaluări
- Cantarella2018 DisyunciónDocument9 paginiCantarella2018 DisyunciónFernando Ruiz BorsiniÎncă nu există evaluări
- Clase IIIDocument14 paginiClase IIIRolando GamarraÎncă nu există evaluări
- Three-Dimensional Evaluation of Maxillary Dentoalveolar Changes and Airway Space After Distalization in AdultsDocument8 paginiThree-Dimensional Evaluation of Maxillary Dentoalveolar Changes and Airway Space After Distalization in AdultsS.g. JorgeÎncă nu există evaluări
- Unilateral ExtractionDocument10 paginiUnilateral ExtractionShatabdi A ChakravartyÎncă nu există evaluări
- Clase III No QuirurgicoDocument8 paginiClase III No QuirurgicoNadia Vite SáenzÎncă nu există evaluări
- Determining Canine PositionDocument28 paginiDetermining Canine PositionMamata DugarajuÎncă nu există evaluări
- 10 1016@j Ajodo 2018 10 018Document10 pagini10 1016@j Ajodo 2018 10 018Maria Alejandra ForeroÎncă nu există evaluări
- Correlacion Entre Patron de Crecimiento Facial y Posicion Del Tercer Molar MandibularDocument7 paginiCorrelacion Entre Patron de Crecimiento Facial y Posicion Del Tercer Molar MandibularLili Arroyo SorianoÎncă nu există evaluări
- Classification of Facial Asymmetry by Cluster Analysis: Original ArticleDocument6 paginiClassification of Facial Asymmetry by Cluster Analysis: Original Articlesajida khanÎncă nu există evaluări
- Treatment of Facial Asymmetry and Severe Midline Deviation With Orthodontic Mini-ImplantsDocument13 paginiTreatment of Facial Asymmetry and Severe Midline Deviation With Orthodontic Mini-ImplantsRicha AhlawatÎncă nu există evaluări
- Asymmetric Deep Bite With A Canted Occlusal Plane - A Case ReportDocument9 paginiAsymmetric Deep Bite With A Canted Occlusal Plane - A Case ReportIacominiGustavoÎncă nu există evaluări
- 4.diagnosis of Facial AsymmetryDocument17 pagini4.diagnosis of Facial AsymmetryKajal Panchal19951995Încă nu există evaluări
- Psychological Well-Being, Dental Esthetics, and Psychosocial Impacts in Adolescent Orthodontic Patients: A Prospective Longitudinal StudyDocument12 paginiPsychological Well-Being, Dental Esthetics, and Psychosocial Impacts in Adolescent Orthodontic Patients: A Prospective Longitudinal StudyMonojit DuttaÎncă nu există evaluări
- Craniofacial Morphology of HIV-positive Children and Adolescents Undergoing Antiretroviral Therapy: A Pilot StudyDocument10 paginiCraniofacial Morphology of HIV-positive Children and Adolescents Undergoing Antiretroviral Therapy: A Pilot StudyMonojit DuttaÎncă nu există evaluări
- Physical Properties of Root Cementum: Part 26. Effects of Micro-Osteoperforations On Orthodontic Root Resorption: A Microcomputed Tomography StudyDocument10 paginiPhysical Properties of Root Cementum: Part 26. Effects of Micro-Osteoperforations On Orthodontic Root Resorption: A Microcomputed Tomography StudyMonojit DuttaÎncă nu există evaluări
- American Journal of Orthodontics and Dentofacial Orthopedics Volume 153 Issue 1 2018 (Doi 10.1016 - J.ajodo.2017.05.024) Uesugi, Shunsuke Kokai, Satoshi Kanno, Zuisei Ono, Takashi - Stability of SDocument7 paginiAmerican Journal of Orthodontics and Dentofacial Orthopedics Volume 153 Issue 1 2018 (Doi 10.1016 - J.ajodo.2017.05.024) Uesugi, Shunsuke Kokai, Satoshi Kanno, Zuisei Ono, Takashi - Stability of SMonojit DuttaÎncă nu există evaluări
- Surgery First Using Skeletal Anchorage With Tandem Mechanics For Mandibular Molar DistalizationDocument13 paginiSurgery First Using Skeletal Anchorage With Tandem Mechanics For Mandibular Molar DistalizationMonojit DuttaÎncă nu există evaluări
- Long-Term Changes of The Anterior Palatal Alveolar Bone After Treatment With Bialveolar Protrusion, Evaluated With Computed TomographyDocument10 paginiLong-Term Changes of The Anterior Palatal Alveolar Bone After Treatment With Bialveolar Protrusion, Evaluated With Computed TomographyMonojit DuttaÎncă nu există evaluări
- Craniofacial Morphology in Women With Class I Occlusion and Severe Maxillary Anterior CrowdingDocument10 paginiCraniofacial Morphology in Women With Class I Occlusion and Severe Maxillary Anterior CrowdingMonojit DuttaÎncă nu există evaluări
- Vertical Control of A Class II Deep Bite Malocclusion With The Use of Orthodontic Mini-ImplantsDocument12 paginiVertical Control of A Class II Deep Bite Malocclusion With The Use of Orthodontic Mini-ImplantsMonojit DuttaÎncă nu există evaluări
- Autotransplantation of Premolars and Space Closure in A Patient With in Amed SinusesDocument12 paginiAutotransplantation of Premolars and Space Closure in A Patient With in Amed SinusesMonojit DuttaÎncă nu există evaluări
- Precision and Trueness of Dental Models Manufactured With Different 3-Dimensional Printing TechniquesDocument10 paginiPrecision and Trueness of Dental Models Manufactured With Different 3-Dimensional Printing TechniquesMonojit DuttaÎncă nu există evaluări
- Item-Level Analysis of The Relationship Between Orthodontic Treatment Need and Oral Health - Related Quality of Life in Korean SchoolchildrenDocument7 paginiItem-Level Analysis of The Relationship Between Orthodontic Treatment Need and Oral Health - Related Quality of Life in Korean SchoolchildrenMonojit DuttaÎncă nu există evaluări
- Yildirim2019 PDFDocument9 paginiYildirim2019 PDFMonojit DuttaÎncă nu există evaluări
- Eastman PDFDocument7 paginiEastman PDFMonojit DuttaÎncă nu există evaluări
- Orthodontics-Periodontics Relationship: Readers' ForumDocument2 paginiOrthodontics-Periodontics Relationship: Readers' ForumMonojit DuttaÎncă nu există evaluări
- American Journal of Orthodontics and Dentofacial Orthopedics Volume 155 Issue 2 2019 (Doi 10.1016 - J.ajodo.2018.03.027) Lacerda Rangel Esper, Maria Ângela Junqueira, Juliana Campos - PhotodynamicDocument11 paginiAmerican Journal of Orthodontics and Dentofacial Orthopedics Volume 155 Issue 2 2019 (Doi 10.1016 - J.ajodo.2018.03.027) Lacerda Rangel Esper, Maria Ângela Junqueira, Juliana Campos - PhotodynamicMonojit DuttaÎncă nu există evaluări
- Comparison of Root Resorption After Bone-Borne and Tooth-Borne Rapid Maxillary Expansion Evaluated With The Use of MicrotomographyDocument9 paginiComparison of Root Resorption After Bone-Borne and Tooth-Borne Rapid Maxillary Expansion Evaluated With The Use of MicrotomographyMonojit DuttaÎncă nu există evaluări
- Lima 2019Document10 paginiLima 2019Monojit DuttaÎncă nu există evaluări
- A Rodent Model Using Skeletal Anchorage and Low Forces For Orthodontic Tooth MovementDocument10 paginiA Rodent Model Using Skeletal Anchorage and Low Forces For Orthodontic Tooth MovementMonojit DuttaÎncă nu există evaluări
- Lee 2019Document7 paginiLee 2019Monojit DuttaÎncă nu există evaluări
- Pharyngeal Airway Evaluation Following Isolated Surgical Mandibular Advancement: A 1-Year Follow-UpDocument9 paginiPharyngeal Airway Evaluation Following Isolated Surgical Mandibular Advancement: A 1-Year Follow-UpMonojit DuttaÎncă nu există evaluări
- 10 1016@j Ajodo 2016 03 020 PDFDocument10 pagini10 1016@j Ajodo 2016 03 020 PDFMonojit DuttaÎncă nu există evaluări
- Asymmettic Space Closure: Clinicians' CornerDocument7 paginiAsymmettic Space Closure: Clinicians' CornerMonojit DuttaÎncă nu există evaluări
- Accelerated Orthodontic Tooth Movement: Molecular MechanismsDocument13 paginiAccelerated Orthodontic Tooth Movement: Molecular MechanismsMonojit DuttaÎncă nu există evaluări
- Extractions, Retention and Stability The Search For Orthodontic Truth Sheldon PeckDocument7 paginiExtractions, Retention and Stability The Search For Orthodontic Truth Sheldon PeckMonojit DuttaÎncă nu există evaluări
- Treatment Planning Assignment - DigmannDocument8 paginiTreatment Planning Assignment - Digmannapi-508053077Încă nu există evaluări
- Oral Mucosal Lesions Indenture WearersDocument27 paginiOral Mucosal Lesions Indenture Wearersade ismailÎncă nu există evaluări
- Medical EmergenciesDocument3 paginiMedical Emergencieskiranvarma2uÎncă nu există evaluări
- Mds Test 2 - RemovedDocument92 paginiMds Test 2 - RemovedSubhashÎncă nu există evaluări
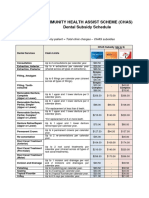
- CHAS Dental Subsidy ScheduleDocument1 paginăCHAS Dental Subsidy ScheduleEugeneÎncă nu există evaluări
- Long-Term Results of Orthodontic Treatment of Impacted Maxillary CaninesDocument8 paginiLong-Term Results of Orthodontic Treatment of Impacted Maxillary CaninesAya Dini Oase CaesarÎncă nu există evaluări
- Infant Oral Health Care PDFDocument5 paginiInfant Oral Health Care PDFITS DENTAL COLLEGE Greater NoidaÎncă nu există evaluări
- Gentle Wave PDFDocument8 paginiGentle Wave PDFcatalinaÎncă nu există evaluări
- NobelReplace Conical Connect OverviewDocument6 paginiNobelReplace Conical Connect Overviewaziz2007Încă nu există evaluări
- Kamatuday Appliance (Triple-Banded Space Regainer) : An Innovative ApplianceDocument3 paginiKamatuday Appliance (Triple-Banded Space Regainer) : An Innovative ApplianceIJAR JOURNALÎncă nu există evaluări
- RCD Midterm Exam Flashcards - QuizletDocument23 paginiRCD Midterm Exam Flashcards - QuizletDENTAL REVIEWER ONLYÎncă nu există evaluări
- Icd-10 Codes For Orthodontics: Introduction - Kirt E. Simmons, DDS, PHDDocument10 paginiIcd-10 Codes For Orthodontics: Introduction - Kirt E. Simmons, DDS, PHDmsk adiwiryaÎncă nu există evaluări
- Oro-Antral CommunicationDocument65 paginiOro-Antral CommunicationNadila RÎncă nu există evaluări
- The Gray Zone Around Dental Implants - Keys To Esthetic SuccessDocument20 paginiThe Gray Zone Around Dental Implants - Keys To Esthetic SuccessZardasht NajmadineÎncă nu există evaluări
- Cavit Ron Plus BrochureDocument11 paginiCavit Ron Plus BrochureIvania Paz Salinas VillanuevaÎncă nu există evaluări
- Ortho Lec - m1 PDFDocument7 paginiOrtho Lec - m1 PDFKaren maeÎncă nu există evaluări
- Notes From The Clinic 1 Phase or 2 PhaseDocument6 paginiNotes From The Clinic 1 Phase or 2 PhaseNizam MuhamadÎncă nu există evaluări
- Dds Guidelines UoftDocument10 paginiDds Guidelines UoftNjhaÎncă nu există evaluări
- Materials and Processes For CAD/CAM Complete Denture FabricationDocument7 paginiMaterials and Processes For CAD/CAM Complete Denture FabricationsamarÎncă nu există evaluări
- A To Z Orthodontics Vol 10 Removable Orthodontic ApplianceDocument34 paginiA To Z Orthodontics Vol 10 Removable Orthodontic ApplianceMa Lyn GabayeronÎncă nu există evaluări
- Space Maintenance: Emma Laing, Paul Ashley, Farhad B. Naini & Daljit S. GillDocument8 paginiSpace Maintenance: Emma Laing, Paul Ashley, Farhad B. Naini & Daljit S. GillAnonymous JR1VNCÎncă nu există evaluări
- Somalia Launches First Ever-Cleft Lip and Palate Surgery ClinicDocument4 paginiSomalia Launches First Ever-Cleft Lip and Palate Surgery ClinicAMISOM Public Information ServicesÎncă nu există evaluări
- Book Reviews: Mandibular Suction-Effective Denture and BPS: A Complete GuideDocument1 paginăBook Reviews: Mandibular Suction-Effective Denture and BPS: A Complete GuideArjun NarangÎncă nu există evaluări
- The Effect of Complete Dentures On Alveolar MucosaDocument8 paginiThe Effect of Complete Dentures On Alveolar MucosaZachary DuongÎncă nu există evaluări
- Clinical Complications of Osseointegrated ImplantsDocument16 paginiClinical Complications of Osseointegrated ImplantsJonathan BalderasÎncă nu există evaluări