S-ar putea să vă placă și
- Laryngopharyngeal and Gastroesophageal Reflux: A Comprehensive Guide to Diagnosis, Treatment, and Diet-Based ApproachesDe la EverandLaryngopharyngeal and Gastroesophageal Reflux: A Comprehensive Guide to Diagnosis, Treatment, and Diet-Based ApproachesCraig H. ZalvanÎncă nu există evaluări
- Benign Migratory Glossitis: A Review: KeywordsDocument11 paginiBenign Migratory Glossitis: A Review: KeywordsDita Merry Diah VanonyÎncă nu există evaluări
- Diagnosis and Treatment of Chronic CoughDe la EverandDiagnosis and Treatment of Chronic CoughSang Heon ChoÎncă nu există evaluări
- Geographic Tongue Literature Review and Case ReportsDocument5 paginiGeographic Tongue Literature Review and Case ReportsafmznqfsclmgbeÎncă nu există evaluări
- Geographic Tongue: Clinical Characteristics of 188 CasesDocument11 paginiGeographic Tongue: Clinical Characteristics of 188 CaseswennyÎncă nu există evaluări
- Geographic TongueDocument5 paginiGeographic Tonguebhawna_aroraÎncă nu există evaluări
- Oral Lichen Planus Clinical Features, Etiology, Treatment andDocument7 paginiOral Lichen Planus Clinical Features, Etiology, Treatment andevhafadlianurÎncă nu există evaluări
- Glositis Dan AtopiDocument6 paginiGlositis Dan AtopiAmanda Rizka PutriÎncă nu există evaluări
- Geographic Tongue: Clinical Characteristics of 188 CasesDocument11 paginiGeographic Tongue: Clinical Characteristics of 188 CasesMahendra PrihandanaÎncă nu există evaluări
- Tongue Lession PrintDocument9 paginiTongue Lession Printdlami_ahÎncă nu există evaluări
- Oral Lichen Planus: Líquen Plano OralDocument11 paginiOral Lichen Planus: Líquen Plano OralFrancielleÎncă nu există evaluări
- 3 Case Report Geographic Tongue Haritsa BudimanDocument10 pagini3 Case Report Geographic Tongue Haritsa Budimanharitsa budimanÎncă nu există evaluări
- Geographic Tongue IsDocument2 paginiGeographic Tongue IsNa DiaÎncă nu există evaluări
- Oral Manifestations of Systemic Diseases A Review, 2014 PDFDocument9 paginiOral Manifestations of Systemic Diseases A Review, 2014 PDFDwi Indah LestariÎncă nu există evaluări
- Halitosis: An Overview of Epidemiology, Etiology and Clinical ManagementDocument6 paginiHalitosis: An Overview of Epidemiology, Etiology and Clinical Managementdrmezzo68Încă nu există evaluări
- Fissured Tongue: A Case Report and Review of Literature: KeywordsDocument5 paginiFissured Tongue: A Case Report and Review of Literature: Keywordssiti baiq gadishaÎncă nu există evaluări
- Manifestasi Oral Nutritional Disorders (Journal)Document12 paginiManifestasi Oral Nutritional Disorders (Journal)yolasrikandiÎncă nu există evaluări
- Enfermedades InmunologicasDocument14 paginiEnfermedades InmunologicasKarina OjedaÎncă nu există evaluări
- Oral Lichenoid Lesions - Distinguishing The Benign From The Deadly (2017)Document14 paginiOral Lichenoid Lesions - Distinguishing The Benign From The Deadly (2017)JohnÎncă nu există evaluări
- 2018 13 (16) No4 pg336-339Document4 pagini2018 13 (16) No4 pg336-339Mihai LupuÎncă nu există evaluări
- Benign Migratory Glossitis and AllergyDocument2 paginiBenign Migratory Glossitis and AllergyAfifah Novita YuliastutiÎncă nu există evaluări
- Oral Lesions in Leprosy Revisited: A Case Report: A. K. Dhawan, MD, Prashant Verma, MD, and S. Sharma, MDDocument2 paginiOral Lesions in Leprosy Revisited: A Case Report: A. K. Dhawan, MD, Prashant Verma, MD, and S. Sharma, MDOjanÎncă nu există evaluări
- Investigation of Volatile Sulfur Compound Level and Halitosis in Patients With Gingivitis and PeriodontitisDocument11 paginiInvestigation of Volatile Sulfur Compound Level and Halitosis in Patients With Gingivitis and PeriodontitisBilly TrầnÎncă nu există evaluări
- Jcad 13 6 48Document6 paginiJcad 13 6 48neetika guptaÎncă nu există evaluări
- Renal Disease and MouthDocument6 paginiRenal Disease and MouthShantanu DixitÎncă nu există evaluări
- Australian Dental Journal - 2010 - Schifter - Oral Mucosal Diseases The Inflammatory DermatosesDocument16 paginiAustralian Dental Journal - 2010 - Schifter - Oral Mucosal Diseases The Inflammatory Dermatosesneetika guptaÎncă nu există evaluări
- PemfigusDocument5 paginiPemfigusSherlyÎncă nu există evaluări
- Occurrence of Recurrent Aphthous Stomatitis (RAS) As A Rare Oral Manifestation in A Patient With Gilbert's SyndromeDocument5 paginiOccurrence of Recurrent Aphthous Stomatitis (RAS) As A Rare Oral Manifestation in A Patient With Gilbert's SyndromeDinesh RokayaÎncă nu există evaluări
- Oral ManifestationDocument18 paginiOral ManifestationDokterGigiÎncă nu există evaluări
- Case Report: Idiopathic Orofacial Granulomatosis With Varied Clinical PresentationDocument4 paginiCase Report: Idiopathic Orofacial Granulomatosis With Varied Clinical PresentationPrince AhmedÎncă nu există evaluări
- Anupdateonfelinechronic Gingivostomatitis: Da Bin Lee,, Frank J.M. Verstraete,, Boaz ArziDocument10 paginiAnupdateonfelinechronic Gingivostomatitis: Da Bin Lee,, Frank J.M. Verstraete,, Boaz ArziAulia FadliahÎncă nu există evaluări
- Oral Manifestations of Systemic Disease: Autoimmune DiseasesDocument7 paginiOral Manifestations of Systemic Disease: Autoimmune DiseaseshussainÎncă nu există evaluări
- Common Oral LesionsDocument13 paginiCommon Oral LesionsFaridaFoulyÎncă nu există evaluări
- Clinical Oral Medicine Lecture NotesDocument3 paginiClinical Oral Medicine Lecture NotesDrMurali G ManoharanÎncă nu există evaluări
- Transfer I RDocument7 paginiTransfer I RAnna Tereza Curado GabeÎncă nu există evaluări
- Symmetry 14 00307Document14 paginiSymmetry 14 00307Phúc BùiÎncă nu există evaluări
- Cheilitis Granulomatosa: Medical Archives January 2011Document3 paginiCheilitis Granulomatosa: Medical Archives January 2011Khairul ArhamÎncă nu există evaluări
- Recurrent Aphthous Ulcerative Disease: Presentation and ManagementDocument6 paginiRecurrent Aphthous Ulcerative Disease: Presentation and ManagementOfier SikiÎncă nu există evaluări
- Todentj 11 539 PDFDocument7 paginiTodentj 11 539 PDFfghdhmdkhÎncă nu există evaluări
- Ilovepdf MergedDocument7 paginiIlovepdf MergedNoval BalanceÎncă nu există evaluări
- Syndromes Palmoplantar KeratodermaDocument6 paginiSyndromes Palmoplantar KeratodermaAdityaEdoÎncă nu există evaluări
- Lyon 2005Document21 paginiLyon 2005Renata StefaniÎncă nu există evaluări
- Recurrent Aphthous Stomatitis: Sunday O. Akintoye, BDS, DDS, MS, Martin S. Greenberg, DDSDocument17 paginiRecurrent Aphthous Stomatitis: Sunday O. Akintoye, BDS, DDS, MS, Martin S. Greenberg, DDSAngga NugrohoÎncă nu există evaluări
- Feline Lymphoplasmacytic Gingivostomatitis: Clinical and Anatomopathological AspectsDocument6 paginiFeline Lymphoplasmacytic Gingivostomatitis: Clinical and Anatomopathological AspectsEzequiel Davi Dos SantosÎncă nu există evaluări
- 4 PDFDocument5 pagini4 PDFLisda PraditaÎncă nu există evaluări
- Hallopeau 10.1001@jamadermatol.2019.3515Document1 paginăHallopeau 10.1001@jamadermatol.2019.3515Faten HayderÎncă nu există evaluări
- Dental Journal: Oral Lesions As A Clinical Sign of Systemic Lupus ErythematosusDocument6 paginiDental Journal: Oral Lesions As A Clinical Sign of Systemic Lupus ErythematosusIin Ardi AÎncă nu există evaluări
- Microbiota LinguaDocument15 paginiMicrobiota LinguaIlana FuxÎncă nu există evaluări
- Prevalence of Periodontal Disease in Children With Leukemia and ThalassemiaDocument14 paginiPrevalence of Periodontal Disease in Children With Leukemia and ThalassemiaZackÎncă nu există evaluări
- Dental JOURNAL: Geographic Tongue in A 6 Year Old Child: A Case Report With Review of LiteratureDocument6 paginiDental JOURNAL: Geographic Tongue in A 6 Year Old Child: A Case Report With Review of LiteraturewennyÎncă nu există evaluări
- Oral Manifestations of SyphilisDocument7 paginiOral Manifestations of SyphilishunarsandhuÎncă nu există evaluări
- Geographic Tongue in Monozygotic Twins: Abst TDocument2 paginiGeographic Tongue in Monozygotic Twins: Abst Twafiqah izzatul auliahÎncă nu există evaluări
- Upsurge of Cases of Lichen Planus in Iraqi Population in Baghdad City With Frequency of Hepatitis VirusesDocument4 paginiUpsurge of Cases of Lichen Planus in Iraqi Population in Baghdad City With Frequency of Hepatitis VirusesIOSRjournalÎncă nu există evaluări
- Leprosy ManualDocument16 paginiLeprosy ManualMikee Laceda NamquiÎncă nu există evaluări
- Riga-Fede Traumatic LingualDocument5 paginiRiga-Fede Traumatic LingualrlagistaÎncă nu există evaluări
- Lom Mer 2013Document17 paginiLom Mer 2013M ElmanavieanÎncă nu există evaluări
- Oral Pemphigus Vulgaris: Corresponding Author: K Subadra, Ksubadra@sriramachandra - Edu.inDocument12 paginiOral Pemphigus Vulgaris: Corresponding Author: K Subadra, Ksubadra@sriramachandra - Edu.inDiva AzariaÎncă nu există evaluări
- Oral Lichen Planus in Children: Case ReportDocument3 paginiOral Lichen Planus in Children: Case ReportFebri YolandaÎncă nu există evaluări
- Scientific Dental Journal: Pigmented Oral Lichen Planus: A Case ReportDocument6 paginiScientific Dental Journal: Pigmented Oral Lichen Planus: A Case ReportSasa AprilaÎncă nu există evaluări
- Geographic Tongue in Psoriasis Case ReportsDocument5 paginiGeographic Tongue in Psoriasis Case Reportsanindita mayaÎncă nu există evaluări
- AG C O L: Uide To Ommon RAL EsionsDocument46 paginiAG C O L: Uide To Ommon RAL EsionsAndykaYayanSetiawanÎncă nu există evaluări
- Produce101s2 PDFDocument22 paginiProduce101s2 PDFwennyÎncă nu există evaluări
- Oral Pathology - Clinical Pathologic Correlations - 6th - EdDocument4 paginiOral Pathology - Clinical Pathologic Correlations - 6th - EdwennyÎncă nu există evaluări
- Podj 3 PDFDocument2 paginiPodj 3 PDFwennyÎncă nu există evaluări
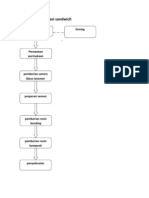
- Prosedur Restorasi SandwichDocument6 paginiProsedur Restorasi SandwichMaria Apriliana100% (1)
- Sist. Urine 2015 2Document37 paginiSist. Urine 2015 2wennyÎncă nu există evaluări
- GypsumDocument14 paginiGypsummuskanÎncă nu există evaluări
- Handbook of Oral Diseases 1 Edition PDFDocument30 paginiHandbook of Oral Diseases 1 Edition PDFwennyÎncă nu există evaluări
- Textbook of Oral Medicine PDFDocument1.179 paginiTextbook of Oral Medicine PDFwenny100% (1)
- Geographic TongueDocument2 paginiGeographic TonguewennyÎncă nu există evaluări
- AG C O L: Uide To Ommon RAL EsionsDocument46 paginiAG C O L: Uide To Ommon RAL EsionsAndykaYayanSetiawanÎncă nu există evaluări
- Immunology Dental CariesDocument24 paginiImmunology Dental CarieswennyÎncă nu există evaluări
- GypsumDocument14 paginiGypsummuskanÎncă nu există evaluări
- 4Document5 pagini4wennyÎncă nu există evaluări
- AG C O L: Uide To Ommon RAL EsionsDocument46 paginiAG C O L: Uide To Ommon RAL EsionsAndykaYayanSetiawanÎncă nu există evaluări
- 4Document5 pagini4wennyÎncă nu există evaluări
- Geographic Tongue and Psoriasis: Clinical, Histopathological, Immunohistochemical and Genetic Correlation - A Literature ReviewDocument12 paginiGeographic Tongue and Psoriasis: Clinical, Histopathological, Immunohistochemical and Genetic Correlation - A Literature ReviewwennyÎncă nu există evaluări
- Dental JOURNAL: Geographic Tongue in A 6 Year Old Child: A Case Report With Review of LiteratureDocument6 paginiDental JOURNAL: Geographic Tongue in A 6 Year Old Child: A Case Report With Review of LiteraturewennyÎncă nu există evaluări
- TheBasicsofBrainWaves - RS PDFDocument4 paginiTheBasicsofBrainWaves - RS PDFOnutu Adriana-LilianaÎncă nu există evaluări
- Etoricoxib - Martindale 39thDocument2 paginiEtoricoxib - Martindale 39thCachimbo PrintÎncă nu există evaluări
- The Practical Reference Guide ForDocument4 paginiThe Practical Reference Guide Forelias667Încă nu există evaluări
- 3 Curvilinear MotionDocument50 pagini3 Curvilinear Motiongarhgelh100% (1)
- 1 Circuit TheoryDocument34 pagini1 Circuit TheoryLove StrikeÎncă nu există evaluări
- ANG DELAVEGA FinalPositionPaperDocument6 paginiANG DELAVEGA FinalPositionPaperZane IbalaÎncă nu există evaluări
- Pellicon 2 Validation Guide PDFDocument45 paginiPellicon 2 Validation Guide PDFtakwahs12135Încă nu există evaluări
- Quartile1 PDFDocument2 paginiQuartile1 PDFHanifah Edres DalumaÎncă nu există evaluări
- Reading Part 2Document14 paginiReading Part 2drama channelÎncă nu există evaluări
- Bchem 455 - Module 3Document42 paginiBchem 455 - Module 3WilliamÎncă nu există evaluări
- Patel 2013Document116 paginiPatel 2013hnphuocÎncă nu există evaluări
- Technical Data Sheet: LPI HVSC PlusDocument2 paginiTechnical Data Sheet: LPI HVSC PlusNguyễn TấnÎncă nu există evaluări
- ELS 06 Maret 223Document16 paginiELS 06 Maret 223Tri WinarsoÎncă nu există evaluări
- Times Square C2C Cardigan: Finished Measurements NotionsDocument8 paginiTimes Square C2C Cardigan: Finished Measurements Notionsdiana.alyÎncă nu există evaluări
- Diagnostic Imaging of The Pharynx and Esophagus: Key PointsDocument33 paginiDiagnostic Imaging of The Pharynx and Esophagus: Key PointsChutcharwan JintasoponÎncă nu există evaluări
- Course Code:TEX3021 Course Title: Wet Processing Technology-IIDocument20 paginiCourse Code:TEX3021 Course Title: Wet Processing Technology-IINakib Ibna BasharÎncă nu există evaluări
- Metal Workers BizHouse - UkDocument3 paginiMetal Workers BizHouse - UkAlex BekeÎncă nu există evaluări
- CulvertsDocument18 paginiCulvertsAmmar A. Ali100% (1)
- Kimi No Na Wa LibropdfDocument150 paginiKimi No Na Wa LibropdfSarangapani BorahÎncă nu există evaluări
- Ap, Lrrsisal of Roentgenograph, Ic: I SsayDocument30 paginiAp, Lrrsisal of Roentgenograph, Ic: I SsayMindaugasStacevičiusÎncă nu există evaluări
- Iso 8033 2016Document9 paginiIso 8033 2016Eric ChuÎncă nu există evaluări
- IBM BladeCenter S RedBookDocument36 paginiIBM BladeCenter S RedBookGuillermo García GándaraÎncă nu există evaluări
- Metaphysics of LucretiusDocument6 paginiMetaphysics of LucretiusChristopher BennettÎncă nu există evaluări
- Electronic Ticket Receipt, January 27 For MS NESHA SIVA SHANMUGAMDocument2 paginiElectronic Ticket Receipt, January 27 For MS NESHA SIVA SHANMUGAMNesha Siva Shanmugam ShavannahÎncă nu există evaluări
- Ict 2120 Animation NC Ii Week 11 20 by Francis Isaac 1Document14 paginiIct 2120 Animation NC Ii Week 11 20 by Francis Isaac 1Chiropractic Marketing NowÎncă nu există evaluări
- Iec60227-3 (Ed2.1) en DDocument6 paginiIec60227-3 (Ed2.1) en Duntuk donlod aaaÎncă nu există evaluări
- RD Sharma Class8 SolutionsDocument2 paginiRD Sharma Class8 Solutionsncertsoluitons100% (2)
- Earth Science Essential Learning Competencies 2020Document5 paginiEarth Science Essential Learning Competencies 2020Charry CervantesÎncă nu există evaluări
- Javanese PeopleDocument22 paginiJavanese PeopleDenisaÎncă nu există evaluări
- FebvreDocument449 paginiFebvreIan Pereira AlvesÎncă nu există evaluări
- The Obesity Code: Unlocking the Secrets of Weight LossDe la EverandThe Obesity Code: Unlocking the Secrets of Weight LossEvaluare: 4 din 5 stele4/5 (5)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsDe la EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsÎncă nu există evaluări
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeDe la EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeEvaluare: 2 din 5 stele2/5 (1)
- The Age of Magical Overthinking: Notes on Modern IrrationalityDe la EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityEvaluare: 4 din 5 stele4/5 (24)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaDe la EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaEvaluare: 4.5 din 5 stele4.5/5 (266)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisDe la EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisEvaluare: 4.5 din 5 stele4.5/5 (42)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedDe la EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedEvaluare: 5 din 5 stele5/5 (80)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDDe la EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDEvaluare: 5 din 5 stele5/5 (1)
- Self-Care for Autistic People: 100+ Ways to Recharge, De-Stress, and Unmask!De la EverandSelf-Care for Autistic People: 100+ Ways to Recharge, De-Stress, and Unmask!Evaluare: 5 din 5 stele5/5 (1)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsDe la EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsEvaluare: 5 din 5 stele5/5 (1)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisDe la EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisEvaluare: 4 din 5 stele4/5 (1)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.De la EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Evaluare: 4.5 din 5 stele4.5/5 (110)
- Gut: the new and revised Sunday Times bestsellerDe la EverandGut: the new and revised Sunday Times bestsellerEvaluare: 4 din 5 stele4/5 (392)
- Why We Die: The New Science of Aging and the Quest for ImmortalityDe la EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityEvaluare: 4 din 5 stele4/5 (3)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsDe la EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsEvaluare: 4.5 din 5 stele4.5/5 (169)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryDe la EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryEvaluare: 4 din 5 stele4/5 (44)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessDe la EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessEvaluare: 4.5 din 5 stele4.5/5 (328)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsDe la EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsEvaluare: 3.5 din 5 stele3.5/5 (3)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisDe la EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisEvaluare: 3.5 din 5 stele3.5/5 (2)
- Sleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningDe la EverandSleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningEvaluare: 4 din 5 stele4/5 (3)
- Gut: The Inside Story of Our Body's Most Underrated Organ (Revised Edition)De la EverandGut: The Inside Story of Our Body's Most Underrated Organ (Revised Edition)Evaluare: 4 din 5 stele4/5 (378)
- To Explain the World: The Discovery of Modern ScienceDe la EverandTo Explain the World: The Discovery of Modern ScienceEvaluare: 3.5 din 5 stele3.5/5 (51)
- The Marshmallow Test: Mastering Self-ControlDe la EverandThe Marshmallow Test: Mastering Self-ControlEvaluare: 4.5 din 5 stele4.5/5 (58)