S-ar putea să vă placă și
- 2015 Immunization Requirements: Frequently Asked QuestionsDocument2 pagini2015 Immunization Requirements: Frequently Asked QuestionsLeonel KongaÎncă nu există evaluări
- Immunization Requirement Form - UpdateDocument2 paginiImmunization Requirement Form - UpdateManojkumar AÎncă nu există evaluări
- Nonmedical Exemption FormDocument1 paginăNonmedical Exemption FormSupreme Understanding DassÎncă nu există evaluări
- Vaccine Exemption FAQs For TexasDocument3 paginiVaccine Exemption FAQs For TexasscribuoyÎncă nu există evaluări
- Immunization FormsDocument8 paginiImmunization FormsJobin JosephÎncă nu există evaluări
- Immunization Requirement - Student Health Center - The University of UtahDocument2 paginiImmunization Requirement - Student Health Center - The University of Utahmithun916Încă nu există evaluări
- PM 286 BDocument2 paginiPM 286 Bnasreen95035Încă nu există evaluări
- Immunization Form For New Students: InstructionsDocument2 paginiImmunization Form For New Students: InstructionskamalÎncă nu există evaluări
- Frequently Asked Questions Vaccine Exemption For Reasons of ConscienceDocument6 paginiFrequently Asked Questions Vaccine Exemption For Reasons of ConscienceRunako RuRu PierceÎncă nu există evaluări
- HCC Health Immunization Application Acknowledgement FormDocument1 paginăHCC Health Immunization Application Acknowledgement FormPhương AnhÎncă nu există evaluări
- Post Secondary School Students NoticeDocument1 paginăPost Secondary School Students NoticeNÃO VEJA MINHA FOTO DE PERFILÎncă nu există evaluări
- Immunization RecordDocument2 paginiImmunization RecordWillÎncă nu există evaluări
- Occupational Health QuestionnaireDocument13 paginiOccupational Health QuestionnaireMohamed HafezÎncă nu există evaluări
- Immunization Record Form Canada ISPDocument1 paginăImmunization Record Form Canada ISPugurgencay62Încă nu există evaluări
- Application For Johns Hopkins Clinical ElectiveDocument1 paginăApplication For Johns Hopkins Clinical ElectiveOsamah ChoudhryÎncă nu există evaluări
- Health Information FormDocument13 paginiHealth Information FormArtero-Cavallaro PabloÎncă nu există evaluări
- HCA+HCAESL+ACCESS - Document ChecklistDocument5 paginiHCA+HCAESL+ACCESS - Document Checklisttajindergrewal100Încă nu există evaluări
- Nursing BSCN Year 1 ERV PackageDocument5 paginiNursing BSCN Year 1 ERV PackageroldinpgÎncă nu există evaluări
- Personal Beliefs Affidavit To Be Signed by Parent or Guardian-TuberculosisDocument1 paginăPersonal Beliefs Affidavit To Be Signed by Parent or Guardian-TuberculosisAkua Ifakórède ElebuibonÎncă nu există evaluări
- WAYNE STATE U Covid Vaccine Declination FormDocument3 paginiWAYNE STATE U Covid Vaccine Declination FormWXYZ-TV Channel 7 DetroitÎncă nu există evaluări
- Univ of Florida ImmunisationDocument2 paginiUniv of Florida ImmunisationPavan Kumar MangipudiÎncă nu există evaluări
- Flu Clinic Admin Record 2022Document2 paginiFlu Clinic Admin Record 2022MATTHEW JONESÎncă nu există evaluări
- Immunization Report PDFDocument2 paginiImmunization Report PDFJag UnathÎncă nu există evaluări
- An Important FormDocument3 paginiAn Important FormRachel ColeÎncă nu există evaluări
- Immunization InstructionsDocument2 paginiImmunization InstructionsAli SadeqiÎncă nu există evaluări
- COVID-19 Vax Consent FormDocument3 paginiCOVID-19 Vax Consent FormCj CCÎncă nu există evaluări
- 2024 VPD FormFINAL 16012024Document5 pagini2024 VPD FormFINAL 16012024dkid9876Încă nu există evaluări
- Physician Certification FormDocument2 paginiPhysician Certification FormSachin Tukaram SalianÎncă nu există evaluări
- Vaccine ExemptionVacLib GeorgiaDocument2 paginiVaccine ExemptionVacLib GeorgiaDonnaÎncă nu există evaluări
- Immunization Titer FormsDocument19 paginiImmunization Titer FormsCole GarrettÎncă nu există evaluări
- Health Immunization Clearance Form: Section A: ImmunizationsDocument3 paginiHealth Immunization Clearance Form: Section A: ImmunizationsFaith SetikÎncă nu există evaluări
- VSLO Immunization Form 22-23Document6 paginiVSLO Immunization Form 22-23Will HÎncă nu există evaluări
- New Idaho Vaccine Exemption FormDocument2 paginiNew Idaho Vaccine Exemption FormDonnaÎncă nu există evaluări
- Emt ApplicationDocument4 paginiEmt ApplicationManuel GonzalezÎncă nu există evaluări
- Health Forms Oct. 2019Document10 paginiHealth Forms Oct. 2019andy hanÎncă nu există evaluări
- Vaccination Exemption Pursuant To Wisconsin Statute 252.04Document2 paginiVaccination Exemption Pursuant To Wisconsin Statute 252.04DonnaÎncă nu există evaluări
- Application Form: 4 Years MD Regular Transfer SeptemberDocument4 paginiApplication Form: 4 Years MD Regular Transfer SeptemberjasjitÎncă nu există evaluări
- ImzformDocument2 paginiImzformapi-509258857Încă nu există evaluări
- Immunization Record: Form Is Due at OrientationDocument3 paginiImmunization Record: Form Is Due at OrientationCasey JonesÎncă nu există evaluări
- Frequently Asked Questions (FAQ) : Communicable Disease Assessment & ImmunizationsDocument6 paginiFrequently Asked Questions (FAQ) : Communicable Disease Assessment & ImmunizationsmaiÎncă nu există evaluări
- Name of Student: Date of Birth: Age: Name of Parent/ Guardian: Address: Contact NumberDocument1 paginăName of Student: Date of Birth: Age: Name of Parent/ Guardian: Address: Contact NumberAlbert RoseteÎncă nu există evaluări
- Request and Certification - Religious Exemption From COVID-19 Vaccine RequirementDocument2 paginiRequest and Certification - Religious Exemption From COVID-19 Vaccine RequirementThe Blackstone ProjectÎncă nu există evaluări
- CUB - Immunisation FormDocument2 paginiCUB - Immunisation FormArcane BeingÎncă nu există evaluări
- MeningococcalDocument2 paginiMeningococcalLuai Sammy Abu-RayyanÎncă nu există evaluări
- FIU Immunization Documentation FormDocument2 paginiFIU Immunization Documentation FormMO MOÎncă nu există evaluări
- Letter Must Be On Faculty Letterhead Date Address Name Date Date Topic (S) of ResearchDocument2 paginiLetter Must Be On Faculty Letterhead Date Address Name Date Date Topic (S) of ResearchCarlos Andrés Pérez-GarzónÎncă nu există evaluări
- 2021-2022 New Student Health Forms - Health ServicesDocument12 pagini2021-2022 New Student Health Forms - Health Servicesnikhil.dharmavaramÎncă nu există evaluări
- Request For Leave of Absence Appeal: Student Number Program (Course)Document2 paginiRequest For Leave of Absence Appeal: Student Number Program (Course)just pocongÎncă nu există evaluări
- SIKAP Medical Certificate Template Filled OutDocument1 paginăSIKAP Medical Certificate Template Filled OutAllen Day100% (1)
- Ohio Provider Guidance Boosters 09.24.21 FINALDocument6 paginiOhio Provider Guidance Boosters 09.24.21 FINALMatt ThomasÎncă nu există evaluări
- Decision To Not Vaccinate My Child: Vaccine / DiseaseDocument2 paginiDecision To Not Vaccinate My Child: Vaccine / DiseaseNano InnaÎncă nu există evaluări
- Sequoia Choice - AZ Distance Learning - Mesa, AZ Vaccine WaiverDocument2 paginiSequoia Choice - AZ Distance Learning - Mesa, AZ Vaccine WaiverDonnaÎncă nu există evaluări
- Pre-Registration Nursing Information For Prospective StudentsDocument4 paginiPre-Registration Nursing Information For Prospective StudentsbthangarajÎncă nu există evaluări
- Immunization FormDocument4 paginiImmunization FormSowmya RaghuÎncă nu există evaluări
- PSW Clinical Requirements Package Fall 2023 InternationalDocument16 paginiPSW Clinical Requirements Package Fall 2023 InternationalAnish KumarÎncă nu există evaluări
- Vaccine RequirementsDocument5 paginiVaccine Requirements卩ㄖ卩卩ㄚ フ乇丂丂丨乇Încă nu există evaluări
- Immunization Waiver FormDocument1 paginăImmunization Waiver Formemmanuel espidaÎncă nu există evaluări
- The Man Behind The Mask: Why I Choose To Not Receive The Flu ShotDe la EverandThe Man Behind The Mask: Why I Choose To Not Receive The Flu ShotÎncă nu există evaluări
- Data Pulse: A Brief Tour of Artificial Intelligence in HealthcareDe la EverandData Pulse: A Brief Tour of Artificial Intelligence in HealthcareÎncă nu există evaluări
- Premed World: Your Journey Toward Medical SchoolDe la EverandPremed World: Your Journey Toward Medical SchoolÎncă nu există evaluări
- Cash Payout Scheme Registration Form (For Cheque Payment To Registrant)Document3 paginiCash Payout Scheme Registration Form (For Cheque Payment To Registrant)karlosgwapo3Încă nu există evaluări
- Cash Payout Scheme Registration Form: (For Direct Bank Transfer To Registrant's Bank Account)Document2 paginiCash Payout Scheme Registration Form: (For Direct Bank Transfer To Registrant's Bank Account)karlosgwapo3Încă nu există evaluări
- Clyde Co - FIDIC Red Book 2017 - A MENA Perspective FINALDocument8 paginiClyde Co - FIDIC Red Book 2017 - A MENA Perspective FINALkarlosgwapo3Încă nu există evaluări
- (2012) Board Resolution - CMS OnlyDocument2 pagini(2012) Board Resolution - CMS Onlykarlosgwapo3Încă nu există evaluări
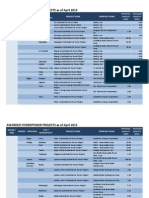
- AwardedHydro2014 01-31Document25 paginiAwardedHydro2014 01-31karlosgwapo3Încă nu există evaluări
- AwardedHydro2013 05-02Document10 paginiAwardedHydro2013 05-02karlosgwapo3Încă nu există evaluări
- The Pyramid PrincipleDocument5 paginiThe Pyramid Principlekarlosgwapo3100% (1)
- Chapter 26Document32 paginiChapter 26karlosgwapo3Încă nu există evaluări
- Bachelor ThesisDocument82 paginiBachelor Thesiskarlosgwapo3Încă nu există evaluări
- ANE BelakangDocument3 paginiANE BelakangGustomo PanantroÎncă nu există evaluări
- Injection Site and Needle Size Vaccine Dose RouteDocument1 paginăInjection Site and Needle Size Vaccine Dose RouteAnonymous vGIfNflwEPÎncă nu există evaluări
- Atención y Funciones Ejecutivas: M.A. Rebollo, S. MontielDocument5 paginiAtención y Funciones Ejecutivas: M.A. Rebollo, S. Montieljonathan smithÎncă nu există evaluări
- Biofarma - PENTAVALENT, One Shot For 5 ProtectionsDocument2 paginiBiofarma - PENTAVALENT, One Shot For 5 ProtectionssarrieÎncă nu există evaluări
- Daftar Pustaka: Nitrition. Maryland: An Aspen PublicationDocument17 paginiDaftar Pustaka: Nitrition. Maryland: An Aspen PublicationrestartÎncă nu există evaluări
- Certificat de Vaccinare Vaccination CertificateDocument1 paginăCertificat de Vaccinare Vaccination CertificateКристина ДолотиноваÎncă nu există evaluări
- Child Immunization Record: Age in Months Nutrional StatusDocument14 paginiChild Immunization Record: Age in Months Nutrional StatusMa. Jesica Salve LasundinÎncă nu există evaluări
- Faktor Risiko Attention Deficit Hyperactivity DisoDocument5 paginiFaktor Risiko Attention Deficit Hyperactivity Disochoco cookiesÎncă nu există evaluări
- SCREENING - ASPERGERS - Children Asperger Screening Tool - CASTDocument6 paginiSCREENING - ASPERGERS - Children Asperger Screening Tool - CASTLana Ako100% (1)
- Laporan Nod Malam TGL 15 Mei 2023Document5 paginiLaporan Nod Malam TGL 15 Mei 2023Yoan Eka Putra PalilingÎncă nu există evaluări
- Expanded Program On ImmunizationDocument7 paginiExpanded Program On ImmunizationkakilalaÎncă nu există evaluări
- National Immunisation Program Schedule Queensland: February 2016Document2 paginiNational Immunisation Program Schedule Queensland: February 2016Anonymous rLmr9GRM2Încă nu există evaluări
- Epi ReviewerDocument4 paginiEpi ReviewerHannah VueltaÎncă nu există evaluări
- Childhood Immunization Schedule 2021Document11 paginiChildhood Immunization Schedule 2021Paula QuiñonesÎncă nu există evaluări
- Pulse Polio - Poster (Eng)Document1 paginăPulse Polio - Poster (Eng)priyankagosbal2006Încă nu există evaluări
- Pentingnya Pemberian Imunisasi DPT Pada Anak Difteri Dan PertusisDocument30 paginiPentingnya Pemberian Imunisasi DPT Pada Anak Difteri Dan Pertusisrevi rillianiÎncă nu există evaluări
- Escoliosis WordDocument9 paginiEscoliosis WordMariano RanalliÎncă nu există evaluări
- Matsne 5094063 17Document54 paginiMatsne 5094063 17Shota JamburidzeÎncă nu există evaluări
- NHS Vaccinations and When To Have Them - NHS PDFDocument1 paginăNHS Vaccinations and When To Have Them - NHS PDFDorota NieradkaÎncă nu există evaluări
- Polio True Story-Rehana: Taken From Polio True Stories TV Series Produced & Directed by Sharp Cut FilmsDocument1 paginăPolio True Story-Rehana: Taken From Polio True Stories TV Series Produced & Directed by Sharp Cut FilmsFurqan MirzaÎncă nu există evaluări
- Fake Vaccines in June 2016Document1 paginăFake Vaccines in June 2016Herlinda SoefiyantiÎncă nu există evaluări
- Daftar Pustaka SpaDocument10 paginiDaftar Pustaka SpaRina PratiwiÎncă nu există evaluări
- Rationalization of AWC Wcdpo SiwanDocument17 paginiRationalization of AWC Wcdpo SiwanAK ContinentalÎncă nu există evaluări
- Data Pendataan Sasaran BayiDocument3 paginiData Pendataan Sasaran Bayibagus wahyuÎncă nu există evaluări
- Deformational Plagiocephaly: A Guide To Diagnosis and TreatmentDocument16 paginiDeformational Plagiocephaly: A Guide To Diagnosis and TreatmentManjunath VaddambalÎncă nu există evaluări
- CH 11 IAP Parental Guide On VaccinationDocument9 paginiCH 11 IAP Parental Guide On VaccinationAkankshaKirtiÎncă nu există evaluări
- MediCard Philippines Naga - List of PediatriciansDocument4 paginiMediCard Philippines Naga - List of PediatriciansJared HaberÎncă nu există evaluări
- Nutrición Del Recién Nacido Sano y Enfermo - Duodécimo Consenso Clínico de La Sociedad Iberoamericana de Neonatología (SIBEN)Document22 paginiNutrición Del Recién Nacido Sano y Enfermo - Duodécimo Consenso Clínico de La Sociedad Iberoamericana de Neonatología (SIBEN)jose alberto gamboa100% (1)
- Polio Phase in Tamil Nadu 2016Document6 paginiPolio Phase in Tamil Nadu 2016Chenthil KumarÎncă nu există evaluări
- Complete VaccinationDocument2 paginiComplete VaccinationNgoo NwosuÎncă nu există evaluări