S-ar putea să vă placă și
- Phys HealthDocument19 paginiPhys HealthJulianna Bartalus100% (1)
- Factor HandoutDocument20 paginiFactor HandoutAbhipreeth MehraÎncă nu există evaluări
- Dissertation PDFDocument253 paginiDissertation PDFsunkissedchiffonÎncă nu există evaluări
- Coping Strategy of Male and Female Grocery Workers - LADocument36 paginiCoping Strategy of Male and Female Grocery Workers - LALawrence Albert MacaraigÎncă nu există evaluări
- Experiences of Parents With Visual Impairments Who Are Raising ChildrenDocument9 paginiExperiences of Parents With Visual Impairments Who Are Raising ChildrenbhezymimzÎncă nu există evaluări
- Burns (2020) - Recommendations in School Psychological Evaluation Reports For Academic DeficitsDocument13 paginiBurns (2020) - Recommendations in School Psychological Evaluation Reports For Academic DeficitssofiaÎncă nu există evaluări
- The International Physical Activity Questionnaire Ipaq A Study of Concurrent and Construct ValidityDocument8 paginiThe International Physical Activity Questionnaire Ipaq A Study of Concurrent and Construct Validityangela_karenina_1Încă nu există evaluări
- Electronic Gadgets Restrains The Children Social Interaction.Document40 paginiElectronic Gadgets Restrains The Children Social Interaction.David Dhea Refazo LinatokÎncă nu există evaluări
- WCCHC Behavioral Health Training ProgramsDocument28 paginiWCCHC Behavioral Health Training Programsjordyn1990Încă nu există evaluări
- A Meta Synthesis of How Parents of Children With Autism Describe Their Experience of Advocating For Their Children During The Process of DiagnosisDocument15 paginiA Meta Synthesis of How Parents of Children With Autism Describe Their Experience of Advocating For Their Children During The Process of DiagnosisKarel Guevara100% (1)
- Students' Level of Metacognitive Awareness As Correlates of Their Mathematics AchievementDocument8 paginiStudents' Level of Metacognitive Awareness As Correlates of Their Mathematics AchievementPsychology and Education: A Multidisciplinary JournalÎncă nu există evaluări
- Autism and Math TalentDocument3 paginiAutism and Math TalentNafisah BaharomÎncă nu există evaluări
- Attachment HandoutsDocument51 paginiAttachment Handoutspreeti17693Încă nu există evaluări
- Global Developmental DelayDocument5 paginiGlobal Developmental DelayMay Pearl NuñalÎncă nu există evaluări
- Measuring Altruism in YouthDocument3 paginiMeasuring Altruism in YouthNazara Aulia100% (1)
- Teen Sleep QuestionnaireDocument3 paginiTeen Sleep QuestionnaireNur fajrina TamimiÎncă nu există evaluări
- Behavioral Family TherapyDocument6 paginiBehavioral Family Therapyiulia9gavrisÎncă nu există evaluări
- Oxford Handbooks Online: Intellectual DisabilitiesDocument20 paginiOxford Handbooks Online: Intellectual DisabilitiesCristina100% (1)
- INTERNET ADDICTION: WHAT IS IT AND HOW CAN IT AFFECT YOUDocument3 paginiINTERNET ADDICTION: WHAT IS IT AND HOW CAN IT AFFECT YOUstuti jainÎncă nu există evaluări
- Most To Least Most To Least: ST ND RD THDocument4 paginiMost To Least Most To Least: ST ND RD THRommel SarjÎncă nu există evaluări
- Model Raoprt Scala MMSEDocument8 paginiModel Raoprt Scala MMSEDiana ArghireÎncă nu există evaluări
- Self Confidence IndiaDocument5 paginiSelf Confidence IndiajosekinÎncă nu există evaluări
- DPC Field Report CompletedDocument36 paginiDPC Field Report Completedraman_bhoomi9910Încă nu există evaluări
- Anxiety and Depression Among Students of A Medical College in Saudi ArabiaDocument6 paginiAnxiety and Depression Among Students of A Medical College in Saudi Arabiahadyan39Încă nu există evaluări
- Relationship between academic achievement and self-esteemDocument5 paginiRelationship between academic achievement and self-esteemaivy rose de ocampo100% (1)
- Effects of Family Functioning and Family Hardiness On Self-Efficacy Among College StudentsDocument9 paginiEffects of Family Functioning and Family Hardiness On Self-Efficacy Among College StudentsSunway UniversityÎncă nu există evaluări
- The Self-Concept According To Gender & Academic Year For Students of Department of Physical Education - Palestine Technical UniversityDocument6 paginiThe Self-Concept According To Gender & Academic Year For Students of Department of Physical Education - Palestine Technical UniversityThe Swedish Journal of Scientific Research (SJSR) ISSN: 2001-9211Încă nu există evaluări
- How to Overcome ProcrastinationDocument20 paginiHow to Overcome ProcrastinationTherk DeshdeepakÎncă nu există evaluări
- Effects of Social Media Effects of Social MediaDocument3 paginiEffects of Social Media Effects of Social MediaWaleed KhanÎncă nu există evaluări
- Pfeiffer, Wong (1989) - Multidimensional Jealousy ScaleDocument17 paginiPfeiffer, Wong (1989) - Multidimensional Jealousy ScaleRoxanaMarin0% (1)
- Management of Childhood and Adolescent DisordersDocument26 paginiManagement of Childhood and Adolescent Disordersdurgesh yadav100% (1)
- Module 3. Unit 1 - The PERMA ModelDocument5 paginiModule 3. Unit 1 - The PERMA ModelNicole Anne ViernesÎncă nu există evaluări
- Parenting Style As A Moderator of Locus of Control, Self Esteem and Academic Stress Among AdolescentsDocument11 paginiParenting Style As A Moderator of Locus of Control, Self Esteem and Academic Stress Among Adolescentsharano mamunÎncă nu există evaluări
- Personal Development 12 AspectsDocument2 paginiPersonal Development 12 AspectsRianne MarieÎncă nu există evaluări
- The University of Lahore, Lahore.: Cerebral PalsyDocument16 paginiThe University of Lahore, Lahore.: Cerebral Palsynosheen murtazaÎncă nu există evaluări
- MQA Psychology Programme StandardsDocument52 paginiMQA Psychology Programme StandardsBella RamliÎncă nu există evaluări
- Intellectual DisabilityDocument22 paginiIntellectual DisabilityMaria CarreñoÎncă nu există evaluări
- The Clock Drawing TestDocument7 paginiThe Clock Drawing Testpetersouisa6454Încă nu există evaluări
- Argument EssayDocument12 paginiArgument Essayapi-5492396560% (1)
- What Is Mental HealthDocument2 paginiWhat Is Mental HealthDoc AlexÎncă nu există evaluări
- 2011 - Windle - What Is Resilience - A Review and Concept AnalysisDocument18 pagini2011 - Windle - What Is Resilience - A Review and Concept AnalysisSilvia RuzÎncă nu există evaluări
- Chapter 2 Conceptualizing Abnormal Psychology PDFDocument67 paginiChapter 2 Conceptualizing Abnormal Psychology PDFGabriel Jeremy OrtegaÎncă nu există evaluări
- Developmental History FormDocument2 paginiDevelopmental History FormocramusÎncă nu există evaluări
- Reading Test - SchizophreniaDocument9 paginiReading Test - SchizophreniaOlive GroupÎncă nu există evaluări
- Juvenile Offenders: What Works? A Summary of Research FindingsDocument22 paginiJuvenile Offenders: What Works? A Summary of Research FindingsWashington State Institute for Public PolicyÎncă nu există evaluări
- Alcohol and Drug Abuse Division (ADAD) Substance Use Disorder Treatment Rules Colorado DHSDocument80 paginiAlcohol and Drug Abuse Division (ADAD) Substance Use Disorder Treatment Rules Colorado DHSBrian HarrisÎncă nu există evaluări
- Clinical Report Psychological MaltreatmentDocument10 paginiClinical Report Psychological Maltreatmentapi-341212290Încă nu există evaluări
- INTRO TO CHILD DEV & EDUCATIONDocument64 paginiINTRO TO CHILD DEV & EDUCATIONRachelle malnawaÎncă nu există evaluări
- SimSensei OverviewDocument1 paginăSimSensei OverviewDom DeSiciliaÎncă nu există evaluări
- Somatoform Disorders: Andre Samosir Vicci PuspaDocument11 paginiSomatoform Disorders: Andre Samosir Vicci PuspaEdwin DarmawanÎncă nu există evaluări
- Classical Theories of Sigmund FreudDocument24 paginiClassical Theories of Sigmund FreudKeona PugaÎncă nu există evaluări
- Challenge The Status QuoDocument49 paginiChallenge The Status QuoChris StewartÎncă nu există evaluări
- Assessement of IntelligenceDocument4 paginiAssessement of IntelligenceSheryl HendersonÎncă nu există evaluări
- Sample Memorandum AgreementDocument4 paginiSample Memorandum AgreementZphike RockhauntÎncă nu există evaluări
- Chapter 7: Mood Disorders and SuicideDocument41 paginiChapter 7: Mood Disorders and SuicideEsraRamosÎncă nu există evaluări
- Applying Structured Teaching Principles To Toilet TrainingDocument18 paginiApplying Structured Teaching Principles To Toilet TrainingMabel FreixesÎncă nu există evaluări
- Internship in Public Health Reflection PaperDocument9 paginiInternship in Public Health Reflection Paperapi-608898269Încă nu există evaluări
- Parental Authority and Its Effects On The Aggression of ChildrenDocument6 paginiParental Authority and Its Effects On The Aggression of ChildrenapjeasÎncă nu există evaluări
- The Quality of Life ScaleDocument15 paginiThe Quality of Life ScaleMohamed Elsayed0% (1)
- Assignment # 2 Quality of Life (QOL) Prepared byDocument6 paginiAssignment # 2 Quality of Life (QOL) Prepared byDental LecturesMMQÎncă nu există evaluări
- Treatment of Trigger Finger by Steroid IDocument3 paginiTreatment of Trigger Finger by Steroid IFayza RihastaraÎncă nu există evaluări
- Keihiteki OpDocument4 paginiKeihiteki OpFayza RihastaraÎncă nu există evaluări
- Epidemiology of Multiple Myeloma: Nikolaus BeckerDocument11 paginiEpidemiology of Multiple Myeloma: Nikolaus BeckerFayza RihastaraÎncă nu există evaluări
- Sickle Cell Anemia A Molecular Disease PDFDocument6 paginiSickle Cell Anemia A Molecular Disease PDFFayza RihastaraÎncă nu există evaluări
- CN - Jurnal Lansia 1Document5 paginiCN - Jurnal Lansia 1vidiaherdinaÎncă nu există evaluări
- 1Document27 pagini1Nada ApriliaÎncă nu există evaluări
- Sickle Cell Anemia A Molecular Disease PDFDocument6 paginiSickle Cell Anemia A Molecular Disease PDFFayza RihastaraÎncă nu există evaluări
- 2017 KDIGO CKD MBD GL Update PDFDocument60 pagini2017 KDIGO CKD MBD GL Update PDFIván HinostrozaÎncă nu există evaluări
- Hematopoietic Reconstitution in A PatienDocument89 paginiHematopoietic Reconstitution in A PatienFayza RihastaraÎncă nu există evaluări
- 1Document27 pagini1Nada ApriliaÎncă nu există evaluări
- Treatment of Trigger Finger by Steroid IDocument3 paginiTreatment of Trigger Finger by Steroid IFayza RihastaraÎncă nu există evaluări
- Canalith Repositioning Procedures Among 965 Patients With Benign Paroxysmal Positional VertigoDocument7 paginiCanalith Repositioning Procedures Among 965 Patients With Benign Paroxysmal Positional VertigoFayza RihastaraÎncă nu există evaluări
- Rubenstein - Falls in The Nursing HomeDocument11 paginiRubenstein - Falls in The Nursing HomeFayza RihastaraÎncă nu există evaluări
- Percutaneous Treatment of Trigger Finger 34 Fingers Followed 0 5 2 YearsDocument3 paginiPercutaneous Treatment of Trigger Finger 34 Fingers Followed 0 5 2 YearsFayza RihastaraÎncă nu există evaluări
- 2017 KDIGO CKD MBD GL Update PDFDocument60 pagini2017 KDIGO CKD MBD GL Update PDFIván HinostrozaÎncă nu există evaluări
- Treatment of Trigger Finger by Steroid IDocument3 paginiTreatment of Trigger Finger by Steroid IFayza RihastaraÎncă nu există evaluări
- Autologous Bone Marrow - Derived Mesenchymal Stem Cells Vs Autologous Chondrocytes ImplantationDocument8 paginiAutologous Bone Marrow - Derived Mesenchymal Stem Cells Vs Autologous Chondrocytes ImplantationFayza RihastaraÎncă nu există evaluări
- Görkem ErtuðrulDocument6 paginiGörkem ErtuðrulFayza RihastaraÎncă nu există evaluări
- Davatchi Et Al. 2011 Mesenchymal Stem Cell Therapy For Knee Osteoarthritis. Preliminary Report of Four Patients2Document6 paginiDavatchi Et Al. 2011 Mesenchymal Stem Cell Therapy For Knee Osteoarthritis. Preliminary Report of Four Patients2Fayza RihastaraÎncă nu există evaluări
- Biomechanical and Neuromuscular EffectsDocument10 paginiBiomechanical and Neuromuscular EffectsFayza RihastaraÎncă nu există evaluări
- Ajhg00558 0047 PDFDocument10 paginiAjhg00558 0047 PDFFayza RihastaraÎncă nu există evaluări
- Abbreviated Mental State Test PDFDocument1 paginăAbbreviated Mental State Test PDFFayza RihastaraÎncă nu există evaluări
- Three-Dimensional Dynamic in Vivo Motion of The Cervical Spine: Assessment of Measurement Accuracy and Preliminary FindingsDocument8 paginiThree-Dimensional Dynamic in Vivo Motion of The Cervical Spine: Assessment of Measurement Accuracy and Preliminary FindingsFayza RihastaraÎncă nu există evaluări
- Accepted ManuscriptDocument17 paginiAccepted ManuscriptFayza RihastaraÎncă nu există evaluări
- A Review of The Acute Effects of StaticDocument19 paginiA Review of The Acute Effects of StaticFayza RihastaraÎncă nu există evaluări
- Biomechanical Comparison of An Interspinous DeviceDocument7 paginiBiomechanical Comparison of An Interspinous DeviceFayza RihastaraÎncă nu există evaluări
- Feasibility of Physical and Occupational Therapy BDocument7 paginiFeasibility of Physical and Occupational Therapy BFayza RihastaraÎncă nu există evaluări
- Accepted ManuscriptDocument17 paginiAccepted ManuscriptFayza RihastaraÎncă nu există evaluări
- 2010marsystemreview PDFDocument9 pagini2010marsystemreview PDFFayza RihastaraÎncă nu există evaluări
- "Virtopsy" Virtual Alternative For Post-Mortem Investigation in Pandemic Era of Covid-19: Diagnostic Approach To Reduce The Menace of Contagion: - A ReviewDocument6 pagini"Virtopsy" Virtual Alternative For Post-Mortem Investigation in Pandemic Era of Covid-19: Diagnostic Approach To Reduce The Menace of Contagion: - A ReviewInternational Journal of Innovative Science and Research TechnologyÎncă nu există evaluări
- NCP - Acute Pain Related To EdemaDocument2 paginiNCP - Acute Pain Related To EdemaChenime Añana0% (1)
- Hyperthyroidism: Case Presentation and DiscussionDocument7 paginiHyperthyroidism: Case Presentation and DiscussionCalingalan Hussin CaluangÎncă nu există evaluări
- Nursing Care Plan ON: Caesarean DeliveryDocument22 paginiNursing Care Plan ON: Caesarean DeliveryKavi rajput79% (14)
- Course Task #3: AnswerDocument5 paginiCourse Task #3: AnswerAria100% (3)
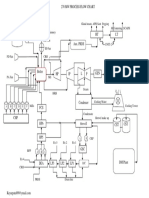
- Power Plant Process Flow Chart PDFDocument1 paginăPower Plant Process Flow Chart PDFFikriHidayatullahÎncă nu există evaluări
- Food Poisoning Presentation FinalDocument20 paginiFood Poisoning Presentation Finalwazeela malikÎncă nu există evaluări
- Chapter 128 - Thyroid and Adrenal Disorders: Episode OverviewDocument15 paginiChapter 128 - Thyroid and Adrenal Disorders: Episode OverviewIkenna EzeiloÎncă nu există evaluări
- Mental Health Importance, Causes, Types & TreatmentsTITLEDocument4 paginiMental Health Importance, Causes, Types & TreatmentsTITLEFatin AfyqahÎncă nu există evaluări
- Akut AbdomenDocument24 paginiAkut AbdomenSelingkuhan neptunusÎncă nu există evaluări
- Updated IDSA - ATS Guidelines On Management of Adults With HAP and VAPDocument11 paginiUpdated IDSA - ATS Guidelines On Management of Adults With HAP and VAPr dwiandiniÎncă nu există evaluări
- Block 4Document106 paginiBlock 4Dr. Megha RichhariyaÎncă nu există evaluări
- Examination Topics - Internal Medicine: Academic Year 2012/2013Document48 paginiExamination Topics - Internal Medicine: Academic Year 2012/2013harisnclÎncă nu există evaluări
- Diseases of CoconutDocument7 paginiDiseases of CoconutKA AngappanÎncă nu există evaluări
- Common Name Scientific Name Origin Plant Botanical Name Chemical ConstituentsDocument1 paginăCommon Name Scientific Name Origin Plant Botanical Name Chemical Constituentscyper zoonÎncă nu există evaluări
- DLC PracticalDocument6 paginiDLC PracticalAngoruz Gohain BaruahÎncă nu există evaluări
- Dosing For Bipolar Mania - Depakote® (Divalproex Sodium)Document6 paginiDosing For Bipolar Mania - Depakote® (Divalproex Sodium)do leeÎncă nu există evaluări
- Ichrak Ghachem, Sabra Riahi, Sana Ben Hmida, Asma Allaya, Samia Younes Department of Neurologie, CHU Taher Sfar MahdiaDocument1 paginăIchrak Ghachem, Sabra Riahi, Sana Ben Hmida, Asma Allaya, Samia Younes Department of Neurologie, CHU Taher Sfar Mahdiaإشراق IchrakÎncă nu există evaluări
- Neurologic ExaminationDocument67 paginiNeurologic Examinationሀይደር ዶ.ር100% (1)
- Spontaneous Hepatic Rupture Associated With HELLP Syndrome: Britt C. Smyth, BA, RDMS, RVT, RDCSDocument3 paginiSpontaneous Hepatic Rupture Associated With HELLP Syndrome: Britt C. Smyth, BA, RDMS, RVT, RDCSMetharisaÎncă nu există evaluări
- Management of Stroke in The NCCUDocument25 paginiManagement of Stroke in The NCCUsaudÎncă nu există evaluări
- Mango Malformation ReviewDocument6 paginiMango Malformation ReviewBhanu DangiÎncă nu există evaluări
- ESRD Causes and StagesDocument63 paginiESRD Causes and StagesGregory LitangÎncă nu există evaluări
- HS 10.2.1 Section 1 Food Safety Policy PDFDocument24 paginiHS 10.2.1 Section 1 Food Safety Policy PDFSpreading KnowledgeÎncă nu există evaluări
- Viro Final 6Document10 paginiViro Final 6Muhammad Arslan UsmanÎncă nu există evaluări
- Orofacial Complications of Non Surgical Cancer TherapyDocument59 paginiOrofacial Complications of Non Surgical Cancer TherapyKassim OboghenaÎncă nu există evaluări
- Kapalbhati PDFDocument2 paginiKapalbhati PDFRahul MishraÎncă nu există evaluări
- Skripsi Samania Ayu Sari IntangDocument47 paginiSkripsi Samania Ayu Sari IntangHaslinda 123100% (1)
- Pediatric Tuberculosis Signs & SymptomsDocument3 paginiPediatric Tuberculosis Signs & SymptomsJeym Quinny ClapanoÎncă nu există evaluări
- Drug CalculationDocument34 paginiDrug CalculationMalathi VarnaÎncă nu există evaluări