S-ar putea să vă placă și
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Linear Algebra Vector - SpaceDocument98 paginiLinear Algebra Vector - SpaceEngr Suleman Memon100% (1)
- Volume 3Document152 paginiVolume 3Ayush Gupta100% (1)
- Mathematics Form 3Document24 paginiMathematics Form 3Amal Sufiah82% (33)
- FormZ - Quick Reference GuideDocument32 paginiFormZ - Quick Reference GuidemercoviciÎncă nu există evaluări
- Incidence GeometryDocument246 paginiIncidence GeometryGiovanni Gatto100% (1)
- Gelfand - Lectures On Linear AlgebraDocument193 paginiGelfand - Lectures On Linear AlgebraVT Wyee100% (8)
- Mansfield Linear Algebra PDFDocument257 paginiMansfield Linear Algebra PDFHerbert BoogieÎncă nu există evaluări
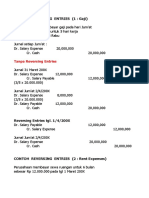
- Contoh Reversing Entries-RevisiDocument8 paginiContoh Reversing Entries-Revisiabdul robby farhanÎncă nu există evaluări
- Materi 1 - Lesi Putih Keratotik, Lesi Praganas Dan GanasDocument76 paginiMateri 1 - Lesi Putih Keratotik, Lesi Praganas Dan Ganasabdul robby farhanÎncă nu există evaluări
- PersediaanDocument31 paginiPersediaanabdul robby farhanÎncă nu există evaluări
- Natha PatDocument1 paginăNatha Patabdul robby farhanÎncă nu există evaluări
- Natha PatDocument1 paginăNatha Patabdul robby farhanÎncă nu există evaluări
- Natha PatDocument1 paginăNatha Patabdul robby farhanÎncă nu există evaluări
- Staffing in Dental PracticeDocument17 paginiStaffing in Dental Practiceabdul robby farhanÎncă nu există evaluări
- Mocha For After Effects Quick Start - ReferenceDocument45 paginiMocha For After Effects Quick Start - ReferenceIann Mae YangaÎncă nu există evaluări
- List of Sheets - Engineering Drawing LabDocument3 paginiList of Sheets - Engineering Drawing LabprashantattÎncă nu există evaluări
- Tool GeometryDocument66 paginiTool Geometrypotnuru JaivanthÎncă nu există evaluări
- c04 Catia v5r15 Sketched Based FeaturesDocument39 paginic04 Catia v5r15 Sketched Based FeaturesMan Scha100% (1)
- Laporan Design 1 Rencana Garis (English)Document107 paginiLaporan Design 1 Rencana Garis (English)Miftah Irfan FirdausiÎncă nu există evaluări
- AnsSol - JEEMain 2023 - PH 2 - 06 04 2023 - Evening Paper PDFDocument21 paginiAnsSol - JEEMain 2023 - PH 2 - 06 04 2023 - Evening Paper PDFArchit SinghaniaÎncă nu există evaluări
- Single Point Turning Tool Page FinalDocument40 paginiSingle Point Turning Tool Page FinalPaulPrateekÎncă nu există evaluări
- Xercise: Jee ProblemsDocument3 paginiXercise: Jee ProblemsAnurag KumarÎncă nu există evaluări
- Analysis of Shannon-Fisher Information Plane in Time Series Based On Information EntropyDocument10 paginiAnalysis of Shannon-Fisher Information Plane in Time Series Based On Information EntropytrolllolfuckubitchÎncă nu există evaluări
- Engineering Math - IIDocument2 paginiEngineering Math - IIAnóòp PaudelÎncă nu există evaluări
- Intersection of Line and PlaneDocument2 paginiIntersection of Line and PlaneAljon AbriamÎncă nu există evaluări
- Basic Curves NXDocument29 paginiBasic Curves NXFidel CruzÎncă nu există evaluări
- MATH10 Lesson 5Document46 paginiMATH10 Lesson 5Bea OroÎncă nu există evaluări
- MA1511 Chapter 3Document20 paginiMA1511 Chapter 3Kang Le LimÎncă nu există evaluări
- Detailed Lesson PlanDocument7 paginiDetailed Lesson PlanJESSA CANOPINÎncă nu există evaluări
- 1898 Are Euclid's Axioms Empirical, RussellDocument8 pagini1898 Are Euclid's Axioms Empirical, RussellAlexandreCFilhoÎncă nu există evaluări
- Modelado de Bobina ChattockDocument7 paginiModelado de Bobina ChattockLeandro AriasÎncă nu există evaluări
- Three Dimensional Geometry PDFDocument2 paginiThree Dimensional Geometry PDFabhinavÎncă nu există evaluări
- Summative Test in Math 8 For Modules 1 and 2Document3 paginiSummative Test in Math 8 For Modules 1 and 2Ruben Padilla Dolor LagueÎncă nu există evaluări
- Mathematics T STPM 2014 Sem 1 Trial Paper SIGSDocument4 paginiMathematics T STPM 2014 Sem 1 Trial Paper SIGSKenneth Chan100% (2)
- Applied Mathematics - 1 - 241221155013Document70 paginiApplied Mathematics - 1 - 241221155013girum sisayÎncă nu există evaluări
- Introduction To Architectural Visual Communication 3Document8 paginiIntroduction To Architectural Visual Communication 3angelle cariagaÎncă nu există evaluări
- Suggested Technique For Creating An Involute GearDocument3 paginiSuggested Technique For Creating An Involute Gearigualdi53Încă nu există evaluări