S-ar putea să vă placă și
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (399)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
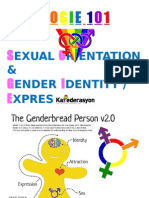
- Sogie 101 7-7-15Document26 paginiSogie 101 7-7-15Murphy Red100% (1)
- MasturbationDocument18 paginiMasturbationRicardo GarciaÎncă nu există evaluări
- Herbal AbortionDocument26 paginiHerbal AbortionMandy M.100% (52)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (73)
- How To Find The PC Muscle For KegelsDocument1 paginăHow To Find The PC Muscle For KegelsDevi LÎncă nu există evaluări
- Neonatal History and Physical ExamDocument2 paginiNeonatal History and Physical ExamMuhammad Farhan KhaliqÎncă nu există evaluări
- Premenstrual Syndrome QuestionnaireDocument4 paginiPremenstrual Syndrome QuestionnaireVoidance 79100% (1)
- Female Reproductive OrgansDocument42 paginiFemale Reproductive Organsaliyah nerz83% (6)
- Antenatal ExercisesDocument11 paginiAntenatal ExercisesRashmi C S0% (1)
- Pourusha VastiDocument54 paginiPourusha Vastiksr prasadÎncă nu există evaluări
- Rising Caesarean Section Rates PosterDocument1 paginăRising Caesarean Section Rates PosteraliasLiewÎncă nu există evaluări
- CT Main Pulm Art DiameterDocument3 paginiCT Main Pulm Art DiameterdrrahulsshindeÎncă nu există evaluări
- Contrast Media and The Kidney European Society ofDocument6 paginiContrast Media and The Kidney European Society ofdrrahulsshindeÎncă nu există evaluări
- Adult Intussusception CT DiagnosisDocument6 paginiAdult Intussusception CT DiagnosisdrrahulsshindeÎncă nu există evaluări
- Lobar AtelectasisDocument9 paginiLobar AtelectasisGusti Ngurah PÎncă nu există evaluări
- Scrotal Calci CationDocument6 paginiScrotal Calci CationdrrahulsshindeÎncă nu există evaluări
- Soft Tissue Tumours and Mass-Like Lesions of The Chest WallDocument7 paginiSoft Tissue Tumours and Mass-Like Lesions of The Chest WalldrrahulsshindeÎncă nu există evaluări
- Colour Doppler Ultrasound Ow Patterns in The Portal VeinDocument11 paginiColour Doppler Ultrasound Ow Patterns in The Portal VeindrrahulsshindeÎncă nu există evaluări
- Sister Mary Joseph NoduleDocument4 paginiSister Mary Joseph NoduledrrahulsshindeÎncă nu există evaluări
- Trigeminal Nerve Anatomy and PathologyDocument10 paginiTrigeminal Nerve Anatomy and PathologydrrahulsshindeÎncă nu există evaluări
- Imaging Features of Pelvic EndometriosisDocument7 paginiImaging Features of Pelvic EndometriosisdrrahulsshindeÎncă nu există evaluări
- Female Genital Tuberculosis HysterosalpingiographyDocument6 paginiFemale Genital Tuberculosis HysterosalpingiographydrrahulsshindeÎncă nu există evaluări
- Imaging of The Petrous ApexDocument9 paginiImaging of The Petrous ApexdrrahulsshindeÎncă nu există evaluări
- Ultrasound Spectrum of Intraductal Papillary NeoplasmsDocument7 paginiUltrasound Spectrum of Intraductal Papillary NeoplasmsdrrahulsshindeÎncă nu există evaluări
- Ultrasound Evaluation of The Brosis Stage in Chronic LiverDocument9 paginiUltrasound Evaluation of The Brosis Stage in Chronic LiverdrrahulsshindeÎncă nu există evaluări
- Vesicoureteric Reflux in The AdultDocument9 paginiVesicoureteric Reflux in The AdultdrrahulsshindeÎncă nu există evaluări
- Cancer Risks From Diagnostic RadiologyDocument17 paginiCancer Risks From Diagnostic RadiologydrrahulsshindeÎncă nu există evaluări
- CT Findings in Pulmonary TuberculosisDocument13 paginiCT Findings in Pulmonary TuberculosisdrrahulsshindeÎncă nu există evaluări
- Spinal Ultrasound in InfantsDocument9 paginiSpinal Ultrasound in InfantsdrrahulsshindeÎncă nu există evaluări
- Contrast Media and The Kidney European Society ofDocument6 paginiContrast Media and The Kidney European Society ofdrrahulsshindeÎncă nu există evaluări
- CT of A Thickened-Wall Gall BladderDocument7 paginiCT of A Thickened-Wall Gall BladderdrrahulsshindeÎncă nu există evaluări
- CT of Duodenal PathologyDocument7 paginiCT of Duodenal PathologydrrahulsshindeÎncă nu există evaluări
- Tubeless Hypotonic DuodenographyDocument12 paginiTubeless Hypotonic DuodenographydrrahulsshindeÎncă nu există evaluări
- Radiographic Assessment of CTEVDocument6 paginiRadiographic Assessment of CTEVdrrahulsshindeÎncă nu există evaluări
- Trigeminal Nerve Anatomy and PathologyDocument10 paginiTrigeminal Nerve Anatomy and PathologydrrahulsshindeÎncă nu există evaluări
- CT of Thoracic Lymph Nodes AnatomyDocument7 paginiCT of Thoracic Lymph Nodes AnatomydrrahulsshindeÎncă nu există evaluări
- CT Scanning of Middle Ear CholesteatomaDocument6 paginiCT Scanning of Middle Ear CholesteatomadrrahulsshindeÎncă nu există evaluări
- Cancer Risks From Diagnostic RadiologyDocument17 paginiCancer Risks From Diagnostic RadiologydrrahulsshindeÎncă nu există evaluări
- Surgical Anatomy PF PNSDocument11 paginiSurgical Anatomy PF PNSdrrahulsshindeÎncă nu există evaluări
- Multiplanar Sinus CT AJRDocument10 paginiMultiplanar Sinus CT AJRdrrahulsshindeÎncă nu există evaluări
- Cervical incompetence: Weakened cervix during pregnancyDocument40 paginiCervical incompetence: Weakened cervix during pregnancyAriaPratamaÎncă nu există evaluări
- Fetal CirculationDocument36 paginiFetal CirculationShfici AdanÎncă nu există evaluări
- Stillbirth Series OverviewDocument38 paginiStillbirth Series OverviewZaroon AhmedÎncă nu există evaluări
- The Question of Sex Education in SchoolsDocument2 paginiThe Question of Sex Education in SchoolsPhoebe FranciscoÎncă nu există evaluări
- Abortion Causes & Types: Presented by DeepakDocument41 paginiAbortion Causes & Types: Presented by DeepakMrs. DeepakÎncă nu există evaluări
- English For Midwifery (Prosus) BaruDocument47 paginiEnglish For Midwifery (Prosus) BaruNagistinaÎncă nu există evaluări
- Adventures With The Pastic ManDocument20 paginiAdventures With The Pastic ManMoroni Gomez BrocaÎncă nu există evaluări
- Obstetrics Case Proforma TemplateDocument4 paginiObstetrics Case Proforma TemplateSwapneelShah100% (1)
- Pre Test CA3 EPI IMCI Mother and Child With Rationale and Answer 2Document20 paginiPre Test CA3 EPI IMCI Mother and Child With Rationale and Answer 2Scarlet GrayÎncă nu există evaluări
- Brochure SPC2023Document3 paginiBrochure SPC2023Edwin KurniawanÎncă nu există evaluări
- Dysfunctional Uterine ContractionDocument2 paginiDysfunctional Uterine ContractionAlphine DalgoÎncă nu există evaluări
- Research ArticleDocument7 paginiResearch ArticleViki AmaliaÎncă nu există evaluări
- Access To Childbirth CareDocument67 paginiAccess To Childbirth CareemeÎncă nu există evaluări
- Jurnal ReadingDocument13 paginiJurnal Readingmeyke potutuÎncă nu există evaluări
- Radcliffe-Brown's Sociology of KinshipDocument3 paginiRadcliffe-Brown's Sociology of KinshipAditya Giri DekaÎncă nu există evaluări
- Concept of Sex and Gender Class NoteDocument4 paginiConcept of Sex and Gender Class NoteShital BadhuÎncă nu există evaluări
- Antenatal Care Guidelines for Pregnancy Screening and Risk FactorsDocument81 paginiAntenatal Care Guidelines for Pregnancy Screening and Risk FactorsDorjee SengeÎncă nu există evaluări
- CoitusDocument22 paginiCoitusFileScanÎncă nu există evaluări
- Gambaran Preeklampsia Berat Dan Eklampsia Ditinjau Dari Faktor Risiko Di Rsup Prof. Dr. R. D. Kandou ManadoDocument5 paginiGambaran Preeklampsia Berat Dan Eklampsia Ditinjau Dari Faktor Risiko Di Rsup Prof. Dr. R. D. Kandou ManadoDyah RatnaÎncă nu există evaluări
- Development of The Male Reproductive System PDFDocument6 paginiDevelopment of The Male Reproductive System PDFJacel JacelÎncă nu există evaluări