S-ar putea să vă placă și
- Purpose Health Equity Report 1Document17 paginiPurpose Health Equity Report 1Clara VolintiruÎncă nu există evaluări
- LEV Medicine - Rejuvenation Research Guest EditorialDocument2 paginiLEV Medicine - Rejuvenation Research Guest EditorialoliverÎncă nu există evaluări
- Evaluation of A Multidisciplinary Lipid Clinic ToDocument11 paginiEvaluation of A Multidisciplinary Lipid Clinic ToBRYAN YESKEL MBAUBEDARIÎncă nu există evaluări
- Drug Discovery and DevelopmentDocument7 paginiDrug Discovery and DevelopmentMónica Adriana Rodríguez CadenaÎncă nu există evaluări
- Das (2018) Universal Delivery of HealthcareDocument5 paginiDas (2018) Universal Delivery of HealthcareWaqasRabbaniÎncă nu există evaluări
- Meredith 2015Document2 paginiMeredith 2015Anindya PutriÎncă nu există evaluări
- Surviving Sepsis Campaign Guidelines 2021 Highlights For The Practicing ClinicianDocument8 paginiSurviving Sepsis Campaign Guidelines 2021 Highlights For The Practicing ClinicianMariah BrownÎncă nu există evaluări
- 1 s2.0 S1567568821000027 MainDocument3 pagini1 s2.0 S1567568821000027 MainDr. RajibÎncă nu există evaluări
- Chapter 4 - The Whole Health Process - 2018 - Integrative MedicineDocument8 paginiChapter 4 - The Whole Health Process - 2018 - Integrative Medicineandre100% (1)
- Future Healthcare Value Based Healthcare Is It The Way Forward 002Document5 paginiFuture Healthcare Value Based Healthcare Is It The Way Forward 002amiraÎncă nu există evaluări
- DI Virtual Health AcceleratedDocument20 paginiDI Virtual Health Acceleratedchetan NÎncă nu există evaluări
- Value Based HealthcareDocument48 paginiValue Based HealthcareAsem Shadid100% (1)
- Bipolar TelepsychiatryDocument10 paginiBipolar TelepsychiatryMaria Von ShaftÎncă nu există evaluări
- ADMET for Medicinal Chemists: A Practical GuideDe la EverandADMET for Medicinal Chemists: A Practical GuideKatya TsaiounÎncă nu există evaluări
- Virologic Failure in HIV: An Updated Clinician’s Guide to Assessment and ManagementDe la EverandVirologic Failure in HIV: An Updated Clinician’s Guide to Assessment and ManagementÎncă nu există evaluări
- Use of Cost-Effectiveness Analysis in Health-Care Resource Allocation Decision-Making: How Are Cost-Effectiveness Thresholds Expected To Emerge?Document11 paginiUse of Cost-Effectiveness Analysis in Health-Care Resource Allocation Decision-Making: How Are Cost-Effectiveness Thresholds Expected To Emerge?Hadi KuriryÎncă nu există evaluări
- Continuity Strategies For Long-Stay PICU Patients: Consensus Statements From The Lucile Packard Foundation PICU Continuity PanelDocument13 paginiContinuity Strategies For Long-Stay PICU Patients: Consensus Statements From The Lucile Packard Foundation PICU Continuity PanelOscar PerezÎncă nu există evaluări
- GX LSHC Dei Global Life Sciences Outlook ReportDocument95 paginiGX LSHC Dei Global Life Sciences Outlook ReportmythonÎncă nu există evaluări
- Mhealth-Innovations SystemstrengtheningtoolsDocument12 paginiMhealth-Innovations SystemstrengtheningtoolshmounguiÎncă nu există evaluări
- JCI Whitepaper Cpgs Closing The GapDocument12 paginiJCI Whitepaper Cpgs Closing The GapMathilda UllyÎncă nu există evaluări
- Roche Products and Diagno.Document132 paginiRoche Products and Diagno.Mahmoud Ahmed100% (2)
- Rational Decision Making in MedicineDocument11 paginiRational Decision Making in MedicineSanti AraratÎncă nu există evaluări
- Clostridium Difficile Infection GuidelinesDocument48 paginiClostridium Difficile Infection GuidelinesGiselle NutuÎncă nu există evaluări
- Rockwood. Theou 2020. Clinical Frailty ScoreDocument6 paginiRockwood. Theou 2020. Clinical Frailty ScoreTomas Andres Bahamondes CordovezÎncă nu există evaluări
- Journal Pone 0250434Document35 paginiJournal Pone 0250434Aklilu FelekeÎncă nu există evaluări
- Health Expectations - 2017 - Vermunt - A Three Goal Model For Patients With Multimorbidity A Qualitative ApproachDocument11 paginiHealth Expectations - 2017 - Vermunt - A Three Goal Model For Patients With Multimorbidity A Qualitative ApproachGUSTAVO VERA REALÎncă nu există evaluări
- Purpose and Process of WHO GuidelineDocument14 paginiPurpose and Process of WHO GuidelineDisshiÎncă nu există evaluări
- IDF T2DM GuidelineDocument123 paginiIDF T2DM GuidelineTile KrispiÎncă nu există evaluări
- Guidelines On Management of Clostridioides Difficile Infection in AdultsDocument48 paginiGuidelines On Management of Clostridioides Difficile Infection in AdultsAntonisÎncă nu există evaluări
- Diagnostic Evidence Cooperatives: Bridging The Valley of Death in Diagnostics DevelopmentDocument3 paginiDiagnostic Evidence Cooperatives: Bridging The Valley of Death in Diagnostics DevelopmentNadia AyuningtiasÎncă nu există evaluări
- Is Management Essential To Improving The Performance and Sustainability of Health Care Systems and Organizations A Systematic Review and A Roadmap For Future StudiesDocument6 paginiIs Management Essential To Improving The Performance and Sustainability of Health Care Systems and Organizations A Systematic Review and A Roadmap For Future StudiesRegina GuzmanÎncă nu există evaluări
- 2058-5241 6 210008Document8 pagini2058-5241 6 210008Muhammad TahirÎncă nu există evaluări
- Self-Reported Adherence To Antiretroviral Therapy in HIV+ Colombian PopulationDocument7 paginiSelf-Reported Adherence To Antiretroviral Therapy in HIV+ Colombian PopulationnukarevaÎncă nu există evaluări
- JamdaDocument8 paginiJamdadds (TMU)Încă nu există evaluări
- Scope Forward: The Future of Gastroenterology Is Now in Your HandsDe la EverandScope Forward: The Future of Gastroenterology Is Now in Your HandsÎncă nu există evaluări
- Comprehensive Geriatric Assessment: British Journal of Hospital Medicine (London, England: 2005) August 2014Document5 paginiComprehensive Geriatric Assessment: British Journal of Hospital Medicine (London, England: 2005) August 2014FadhilannisaÎncă nu există evaluări
- Definición Del Concepto EnfermedadDocument4 paginiDefinición Del Concepto EnfermedadMarianela Vásquez ArayaÎncă nu există evaluări
- Multi Stakeholder Consensus On A Target Product Profile For - 2021 - The LancetDocument9 paginiMulti Stakeholder Consensus On A Target Product Profile For - 2021 - The LancetRachelÎncă nu există evaluări
- Novel Design and Analysis For Rare Disease Drug deDocument18 paginiNovel Design and Analysis For Rare Disease Drug deilum.rononÎncă nu există evaluări
- Global Guideline For Type 2 DiabetesDocument123 paginiGlobal Guideline For Type 2 Diabetesdiabetes asiaÎncă nu există evaluări
- Aao Retina y VitreoDocument20 paginiAao Retina y VitreoRaúl Plasencia SaliniÎncă nu există evaluări
- Traumatic Brain Injury Advances Since 2017: What Has Changed?Document2 paginiTraumatic Brain Injury Advances Since 2017: What Has Changed?Stavya DubeyÎncă nu există evaluări
- Application of Health Technology Assessment For Oncology Care in IndiaDocument5 paginiApplication of Health Technology Assessment For Oncology Care in Indialaxman kavitkarÎncă nu există evaluări
- DI - Intelligent Clinical TrialsDocument36 paginiDI - Intelligent Clinical TrialsPKÎncă nu există evaluări
- Understanding The Opportunity CostsDocument3 paginiUnderstanding The Opportunity CostsNasoni RokoÎncă nu există evaluări
- A Model For The Implementation of Lean Improvements in Healthcare Environments As Applied in A Primary Care CenterDocument30 paginiA Model For The Implementation of Lean Improvements in Healthcare Environments As Applied in A Primary Care CenterJhonattan AntonÎncă nu există evaluări
- The Global HIV Epidemics among People Who Inject DrugsDe la EverandThe Global HIV Epidemics among People Who Inject DrugsÎncă nu există evaluări
- SEAR 2022 AMS Webinar Series - 10th - Dec 22Document1 paginăSEAR 2022 AMS Webinar Series - 10th - Dec 22ingrid devi carissaÎncă nu există evaluări
- Yusnita Sri Lestari - HPHE 11Document11 paginiYusnita Sri Lestari - HPHE 11012211050Încă nu există evaluări
- Toma de Decisiones MedicinaDocument13 paginiToma de Decisiones MedicinaKevin Mora BañosÎncă nu există evaluări
- Clostridium Ghid 2017Document48 paginiClostridium Ghid 2017Cristina PironÎncă nu există evaluări
- Deloitte Personalised Medicine Analysis-PGx-ROIDocument32 paginiDeloitte Personalised Medicine Analysis-PGx-ROISimranjit SinghÎncă nu există evaluări
- Captura de Tela 2023-09-08 À(s) 09.17.35Document26 paginiCaptura de Tela 2023-09-08 À(s) 09.17.35Isabela Di PardiÎncă nu există evaluări
- VAP 2 (Kejadian VAP Eropa)Document8 paginiVAP 2 (Kejadian VAP Eropa)tami ariyasraÎncă nu există evaluări
- P 19-35 Liability and Quality Issues in Health Case Fifth EditionDocument30 paginiP 19-35 Liability and Quality Issues in Health Case Fifth EditionbillÎncă nu există evaluări
- Cix 1085Document48 paginiCix 1085Yahia HassaanÎncă nu există evaluări
- Advanced Practice and Leadership in Radiology NursingDe la EverandAdvanced Practice and Leadership in Radiology NursingKathleen A. GrossÎncă nu există evaluări
- Rectus Diastais Guidelines Full TextDocument14 paginiRectus Diastais Guidelines Full TextlakshitÎncă nu există evaluări
- Strengthening Cost-Effectiveness Analysis For Public Health PolicyDocument7 paginiStrengthening Cost-Effectiveness Analysis For Public Health Policypintoa_1Încă nu există evaluări
- VACCINES Brief 1Document8 paginiVACCINES Brief 1Cristina0lk8g NedelcuÎncă nu există evaluări
- DC 6 Digital Gov Data Sheet PDFDocument4 paginiDC 6 Digital Gov Data Sheet PDFCarlos MajanoÎncă nu există evaluări
- Siebel Certification QBankDocument85 paginiSiebel Certification QBankSoj SurajÎncă nu există evaluări
- Opening Ving Card LocksDocument1 paginăOpening Ving Card LocksFilipe FernandesÎncă nu există evaluări
- Brosur Afias 6 NewDocument2 paginiBrosur Afias 6 NewAkbar SetiawanÎncă nu există evaluări
- Microwave ExperimentDocument18 paginiMicrowave ExperimentChris RaymondÎncă nu există evaluări
- Practice ZAcademy Excel NewiesModeDocument9 paginiPractice ZAcademy Excel NewiesModedadang hermawanÎncă nu există evaluări
- Van Der WallsDocument24 paginiVan Der WallsAnonymous oVRvsdWzfBÎncă nu există evaluări
- RCDC Getting StartedDocument13 paginiRCDC Getting StartedEr Suresh Kumar100% (2)
- Template - OQ - 0001 - 01 - Operational Qualification TemplateDocument9 paginiTemplate - OQ - 0001 - 01 - Operational Qualification TemplateSoon Kooi0% (1)
- Admin JobsDocument4 paginiAdmin JobsLakshmann ChettiarÎncă nu există evaluări
- MDC CGK: Aji / Adnan Bayu MRDocument1 paginăMDC CGK: Aji / Adnan Bayu MRDivya NenaÎncă nu există evaluări
- Manjula Kumari.Document5 paginiManjula Kumari.Sanjay KaithwasÎncă nu există evaluări
- Powerstar Programmable InverterDocument92 paginiPowerstar Programmable InverterbhaskarjalanÎncă nu există evaluări
- Recoletos School of Theology: University of Santo Tomas (Manila)Document1 paginăRecoletos School of Theology: University of Santo Tomas (Manila)Aeb Asib Gbhert0% (1)
- Top Best Practices SSISDocument10 paginiTop Best Practices SSISYurkÎncă nu există evaluări
- ComfortClass S407 USADocument20 paginiComfortClass S407 USAPhilippine Bus Enthusiasts SocietyÎncă nu există evaluări
- CIDAM TemplateDocument2 paginiCIDAM TemplateAntonio C. Cayetano100% (2)
- Second Serial Interface of The S5-95U Programmable ControllerDocument109 paginiSecond Serial Interface of The S5-95U Programmable ControllerDugPigeonÎncă nu există evaluări
- ABB-Handbook Protection and Control DevicesDocument157 paginiABB-Handbook Protection and Control DevicesJose Antonio Ramirez MurilloÎncă nu există evaluări
- Prgframe Without OpDocument63 paginiPrgframe Without Opnitin100% (1)
- Lesson Plan 2 Like TermsDocument8 paginiLesson Plan 2 Like Termsapi-245950665Încă nu există evaluări
- 9.2.1.11 Packet Tracer - Configuring Named Standard ACLs Luis SanchezDocument4 pagini9.2.1.11 Packet Tracer - Configuring Named Standard ACLs Luis Sanchezrafael8214Încă nu există evaluări
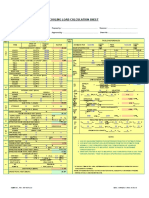
- Cooling Load Calculation Sheet: X X X X X X X X X X X X X X X X Cfm/Person Cfm/DoorDocument6 paginiCooling Load Calculation Sheet: X X X X X X X X X X X X X X X X Cfm/Person Cfm/Doorashfaq-matte-799375% (4)
- Roslyn Riley ResumeDocument2 paginiRoslyn Riley Resumeapi-78443823Încă nu există evaluări
- 1 Historical AntecedentsDocument12 pagini1 Historical AntecedentshithereÎncă nu există evaluări
- HMC 045Document12 paginiHMC 045Mohamed ElmakkyÎncă nu există evaluări
- 113 14Document8 pagini113 14rahul srivastavaÎncă nu există evaluări
- Invoice 02Document2 paginiInvoice 02lobepoj830Încă nu există evaluări
- StepShot User GuideDocument46 paginiStepShot User GuideDeep SachdevaÎncă nu există evaluări
- Low Power CMOS VLSI Design: Aditya Japa Assistant Professor (ECE) KL Hyderabad 12/07/2021Document14 paginiLow Power CMOS VLSI Design: Aditya Japa Assistant Professor (ECE) KL Hyderabad 12/07/2021karthikÎncă nu există evaluări