S-ar putea să vă placă și
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- Introduction To Food Science Edited 15. 09.2019Document37 paginiIntroduction To Food Science Edited 15. 09.2019Jessica chi100% (1)
- Name - Grammar Test SolutionDocument3 paginiName - Grammar Test SolutionABIODUN MicahÎncă nu există evaluări
- Identification and Analysis of Risk ManagementDocument16 paginiIdentification and Analysis of Risk ManagementABIODUN MicahÎncă nu există evaluări
- Risk Management Lesson 1Document8 paginiRisk Management Lesson 1ABIODUN MicahÎncă nu există evaluări
- Read Me (Important)Document2 paginiRead Me (Important)ABIODUN MicahÎncă nu există evaluări
- A Review of Nigeria's 2017 Budget of Recovery & GrowthDocument4 paginiA Review of Nigeria's 2017 Budget of Recovery & GrowthABIODUN MicahÎncă nu există evaluări
- Nigeria's Economy and Recession-Outlook For 2017 RTC Business and Economic Review October 2016Document63 paginiNigeria's Economy and Recession-Outlook For 2017 RTC Business and Economic Review October 2016ABIODUN MicahÎncă nu există evaluări
- Selection and Formulation of Balance DietDocument10 paginiSelection and Formulation of Balance DietNrs Sani Sule MashiÎncă nu există evaluări
- Ecobiol Aqua - A Unique and Highly Effective Single Strain ProbioticDocument5 paginiEcobiol Aqua - A Unique and Highly Effective Single Strain ProbioticInternational Aquafeed magazineÎncă nu există evaluări
- A History of NutritionDocument4 paginiA History of NutritionPramod PradhanÎncă nu există evaluări
- Owner S Manual: Questions?Document16 paginiOwner S Manual: Questions?Marc SchwartzÎncă nu există evaluări
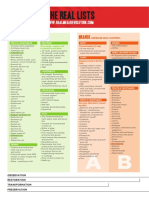
- Real Meal RevolutionTHE-LIST-A4Document2 paginiReal Meal RevolutionTHE-LIST-A4fridayschild2012Încă nu există evaluări
- How To Prevent Flatulence (Aerophagy)Document7 paginiHow To Prevent Flatulence (Aerophagy)krishnaÎncă nu există evaluări
- Hatching and Growth Performances of Guinea Fowl Under Intensive Management SystemDocument9 paginiHatching and Growth Performances of Guinea Fowl Under Intensive Management SystemKadipo BandaÎncă nu există evaluări
- Lifegear 97370Document36 paginiLifegear 97370mrmachÎncă nu există evaluări
- Performance of Free-Range Broiler ChickensDocument8 paginiPerformance of Free-Range Broiler ChickensOliver TalipÎncă nu există evaluări
- Business PlanDocument4 paginiBusiness Plannainaa18Încă nu există evaluări
- Catering SystemsDocument113 paginiCatering SystemsLeslie Mark DacioÎncă nu există evaluări
- Manual ElipticaDocument20 paginiManual ElipticagiovannybsÎncă nu există evaluări
- Cellsentials Vita AntioxidantsDocument1 paginăCellsentials Vita AntioxidantsJulie EdenÎncă nu există evaluări
- Olive Oil As A Functional FoodDocument19 paginiOlive Oil As A Functional FoodRadwan Ajo100% (1)
- Diet JourneyDocument10 paginiDiet JourneyEllyÎncă nu există evaluări
- Chem 441 LAfallanatics Expt 7 BDocument46 paginiChem 441 LAfallanatics Expt 7 Bakifuji913Încă nu există evaluări
- Albumin in Liver Cirrhosis, SADocument37 paginiAlbumin in Liver Cirrhosis, SADwinita ViviantiÎncă nu există evaluări
- PBL Thematic - 3Document9 paginiPBL Thematic - 3Rakshith KumarÎncă nu există evaluări
- Adherence To Iron Folate and Associated Factors Among Pregnant WomenDocument9 paginiAdherence To Iron Folate and Associated Factors Among Pregnant WomenBICARA JIWAÎncă nu există evaluări
- 52 Week Weight Loss ProgramDocument101 pagini52 Week Weight Loss ProgramMartin Schiodtz75% (4)
- Fast Food Restaurants Impact On PeopleDocument6 paginiFast Food Restaurants Impact On PeopleVisa RanicoÎncă nu există evaluări
- Angga Pratama Haloho - 2003511035 - Abstract Assigment - Class ADocument3 paginiAngga Pratama Haloho - 2003511035 - Abstract Assigment - Class AChristmas14 ManjorangFMIPAÎncă nu există evaluări
- CLFTC May 2016 PDFDocument330 paginiCLFTC May 2016 PDFandrewmmwilmotÎncă nu există evaluări
- Surgery 1.04 Surgical Diseases of The Thyroid GlandDocument15 paginiSurgery 1.04 Surgical Diseases of The Thyroid GlandjayaeroneÎncă nu există evaluări
- Lecture 11 Failure To Thrive (FTT)Document25 paginiLecture 11 Failure To Thrive (FTT)jaish8904100% (2)
- Nursing Research Synthesis Paper - 1Document8 paginiNursing Research Synthesis Paper - 1api-308407014Încă nu există evaluări
- Malnutrition: Intervention Plan Nursing Intervention Method of Nurse Family Contact Resource RequiredDocument1 paginăMalnutrition: Intervention Plan Nursing Intervention Method of Nurse Family Contact Resource RequiredSareno PJhēaÎncă nu există evaluări
- Liver Cirrhosis Powerpoint (Week 2) REVISEDDocument33 paginiLiver Cirrhosis Powerpoint (Week 2) REVISEDJustin CacheroÎncă nu există evaluări
- Experiment No. 10 - Fermented Green MangoesDocument2 paginiExperiment No. 10 - Fermented Green MangoesMary Rose CatalbasÎncă nu există evaluări