Documente Academic
Documente Profesional
Documente Cultură
2014 - Nallasamy Et Al. - Low-Dose Vs Standard-Dose Insulin in Pediatric Diabetic Ketoacidosis A Randomized Clinical Trial
Încărcat de
Neha OberoiTitlu original
Drepturi de autor
Formate disponibile
Partajați acest document
Partajați sau inserați document
Vi se pare util acest document?
Este necorespunzător acest conținut?
Raportați acest documentDrepturi de autor:
Formate disponibile
2014 - Nallasamy Et Al. - Low-Dose Vs Standard-Dose Insulin in Pediatric Diabetic Ketoacidosis A Randomized Clinical Trial
Încărcat de
Neha OberoiDrepturi de autor:
Formate disponibile
Research
Original Investigation
Low-Dose vs Standard-Dose Insulin in Pediatric
Diabetic Ketoacidosis
A Randomized Clinical Trial
Karthi Nallasamy, MD, DM; Muralidharan Jayashree, MD; Sunit Singhi, MD; Arun Bansal, MD
Editorial page 990
IMPORTANCE The standard recommended dose (0.1 U/kg per hour) of insulin in diabetic Journal Club Slides and
ketoacidosis (DKA) guidelines is not backed by strong clinical evidence. Physiologic Supplemental content at
dose-effect studies have found that even lower doses could adequately normalize ketonemia jamapediatrics.com
and acidosis. Lowering the insulin dose may be advantageous in the initial hours of therapy
CME Quiz at
when a gradual decrease in glucose, electrolytes, and resultant osmolality is desired. jamanetworkcme.com and
CME Questions page 1083
OBJECTIVE To compare the efficacy and safety of low-dose insulin against the standard dose
in children with DKA.
DESIGN, SETTING, AND PARTICIPANTS This was a prospective, open-label randomized clinical
trial conducted in the pediatric emergency department and intensive care unit of a tertiary
care teaching hospital in northern India from November 1, 2011, through December 31, 2012.
A total of 50 consecutive children 12 years or younger with a diagnosis of DKA were
randomized to low-dose (n = 25) and standard-dose (n = 25) groups.
INTERVENTIONS Low-dose (0.05 U/kg per hour) vs standard-dose (0.1 U/kg per hour) insulin
infusion.
MAIN OUTCOMES AND MEASURES The primary outcome was the rate of decrease in blood
glucose until a level of 250 mg/dL or less is reached (to convert to millimoles per liter,
multiply by 0.0555). The secondary outcomes included time to resolution of acidosis,
episodes of treatment failures, and incidences of hypokalemia and hypoglycemia.
RESULTS The mean (SD) rate of blood glucose decrease until a level of 250 mg/dL or less is
reached (45.1 [17.6] vs 52.2 [23.4] mg/dL/h) and the mean (SD) time taken to achieve this
target (6.0 [3.3] vs 6.2 [2.2] hours) were similar in the low- and standard-dose groups,
respectively. Mean (SD) length of time to achieve resolution of acidosis (low vs standard dose:
16.5 [7.2] vs 17.2 [7.7] hours; P = .73) and rate of resolution of acidosis were also similar in the
groups. Hypokalemia was seen in 12 children (48%) receiving the standard dose vs 5 (20%) of
those receiving the low dose (P = .07); the tendency was more pronounced in malnourished
children (7 [88%] vs 2 [28%]). Five children (20%) and 1 child (4%) receiving standard- and
low-dose infusion (P = .17), respectively, developed hypoglycemia. Treatment failure was rare
and comparable. One child in the standard-dose group developed cerebral edema, and no
deaths occurred during the study period.
CONCLUSIONS AND RELEVANCE Low dose is noninferior to standard dose with respect to rate
of blood glucose decrease and resolution of acidosis. We advocate a superiority trial with a
larger sample size before 0.05 U/kg per hour replaces 0.1 U/kg per hour in the practice
recommendations. Author Affiliations: Department of
Pediatrics, Postgraduate Institute of
Medical Education and Research,
TRIAL REGISTRATION ctri.nic.in Identifier: CTRI/2012/04/002548
Chandigarh, India.
Corresponding Author:
Muralidharan Jayashree, MD,
Department of Pediatrics,
Postgraduate Institute of Medical
Education and Research, Sector 12,
JAMA Pediatr. 2014;168(11):999-1005. doi:10.1001/jamapediatrics.2014.1211 Chandigarh, India 160012
Published online September 29, 2014. (mjshree@hotmail.com).
999
Copyright 2014 American Medical Association. All rights reserved.
Downloaded From: http://archpedi.jamanetwork.com/ by a University of California - San Francisco User on 03/20/2015
Research Original Investigation Insulin in Pediatric Diabetic Ketoacidosis
D
iabetic ketoacidosis (DKA) accounts for 8% to 29% of all search. Written informed consent was obtained from the par-
primary diabetic admissions to a hospital, thus contrib- ents. This was a prospective, open-label randomized clinical
uting to high costs of care for children with type 1 trial conducted in the pediatric emergency department and in-
diabetes mellitus.1 Fluid correction and insulin therapy are the tensive care unit of a tertiary care teaching hospital from No-
cornerstones of DKA management. Although rehydration alone vember 1, 2011, through December 31, 2012. All consecutive chil-
can cause partial correction of hyperglycemia, insulin is required dren 12 years or younger who presented with DKA defined as
to normalize hyperglycemia and suppress lipolysis and hyperglycemia (BG >200 mg/dL [to convert to millimoles per
ketogenesis.2 Insulin therapy has evolved during 4 decades in liter, multiply by 0.0555]), acidosis (pH <7.3 or bicarbonate <15
an attempt to identify a perfect dose that will not only correct mEq/L [to convert to millimoles per liter, multiply by 1]), and
ketoacidosis but also do so without complications. The earlier ketonuria (urine dipstick test result ≥2+) were enrolled.7 Chil-
high-dose (1 U/kg per hour) and bolus insulin therapies went out dren with symptomatic cerebral edema, septic shock at pre-
of vogue after studies3-5 indicated that a similar therapeutic re- sentation, anuria for longer than 6 hours, and insulin treat-
sponse, albeit with minimal adverse effects, could be achieved ment before admission were excluded.
with a dose of 0.1 U/kg per hour. Thereafter, continuous insu-
lin infusion at 0.1 U/kg per hour became standard of care in the Randomization
management of DKA despite not having strong clinical evidence Eligible children were enrolled at 1 hour of admission after re-
of its superiority over lower doses.6,7 A few articles8-10 have high- ceiving the rehydrating fluid during the first hour. A web-
lighted the utility of insulin doses lower than the standard rec- generated random number sequence was used to randomize
ommended one. Noyes et al8 observed that insulin doses of 0.03 them into 2 groups.15 The allocation was concealed in opaque,
and 0.05 U/kg per hour could adequately normalize ketosis in brown, sealed envelopes, which were kept with a health care
DKA. Puttha et al9 and Al Hanshi and Shann,10 in their respec- worker not involved in any other aspect of the study. The pa-
tive pediatric studies, have reported that a dose of 0.05 U/kg per tient assignment was made by opening the numbered enve-
hour was as effective as the standard dose in correcting acidosis. lopes only after obtaining written informed consent. Each en-
It is a well-established fact that resolution of acidosis and not velope contained a slip that listed I (for the low-dose protocol)
blood glucose (BG) reduction determines the end point of DKA or II (for standard-dose protocol). The participants and those
therapy. However, much of the discussion in DKA management administering the interventions were, however, not masked
throughout the years has centered around the initial hours of to group assignment.
therapy, with a focus on sodium, water, BG decrease, and their
effect on rapid osmolar shifts. Although rapid BG decrease by it- Intervention
self has not been conclusively proven to be a risk factor for ce- Insulin therapy was started as a continuous intravenous infu-
rebral edema, some authors have reported a rapid decrease in BG sion using an infusion pump. The low-dose group received
with the use of doses greater than 0.05 U/kg per hour.11 In addi- regular insulin at 0.05 U/kg per hour, whereas the standard-
tion, some have found a more gradual reduction in plasma os- dose group received insulin at 0.1 U/kg per hour. Correction
molality due to slower decrease in BG in children treated with of acidosis (pH ≥7.3 and bicarbonate ≥15 mEq/L) was taken as
0.05 U/kg per hour compared with 0.1 U/kg per hour of insulin.10 the end point, and patients thereafter were shifted to subcu-
The insulin-induced intracellular shift of glucose results in a non- taneous regular insulin with an overlap of 30 minutes.
equimolar increase in serum sodium; the sodium level increases
less than the BG level decreases. Rapid BG decreases can cause Procedures
an attenuated increase in serum sodium, producing a greater than Patients were managed as per the unit’s current protocol for
expected decrease in osmolality.12 Therefore, some authors be- DKA. Fluid volume was calculated as a sum of deficit (65 mL/
lieve that lowering or delaying the insulin dose may cause a kg) and maintenance for 36 hours. Children who presented with
gradual decrease in BG10 and a gentle electrolyte shift.13 More- evidence of hypoperfusion or hypotensive shock received an
over, in developing economies, children with DKA may also ben- additional 20 mL/kg of isotonic saline for 1 hour. Isotonic (0.9%)
efit from a lower insulin dose because associated comorbidities, saline was used as rehydrating fluid for at least the initial 6
such as malnutrition, carry a high risk of therapy-related hypo- hours and changed to half normal (0.45%) saline based on se-
kalemia and hypoglycemia.14 Given this background and the lack rum sodium and corresponding effective osmolality. Dex-
of prospective studies testing lower insulin dose, we planned this trose (5%) was added to rehydrating fluid once the BG level de-
trial to compare low-dose with standard-dose insulin with respect creased to 250 mg/dL or less and the concentration titrated to
to rate of BG decrease, time to resolution of acidosis, episodes maintain a BG level between 180 and 220 mg/dL. Potassium
of treatment failure, and incidence of hypokalemia and hypogly- chloride (40 mEq/L) was added to rehydrating fluid immedi-
cemia in children with DKA. ately after resuscitation to maintain a serum potassium level
between 3.5 and 5.5 mEq/L (to convert to millimoles per liter,
multiply by 1).
Methods
Monitoring
Study Design and Participants Capillary or venous BG was checked every hour or more fre-
The study was approved by the Institute Ethics Committee of quently, depending on clinical need (Optium Xceed glucom-
the Postgraduate Institute of Medical Education and Re- eter; Abbott Diabetes Care Inc). Readings above the glucom-
1000 JAMA Pediatrics November 2014 Volume 168, Number 11 jamapediatrics.com
Copyright 2014 American Medical Association. All rights reserved.
Downloaded From: http://archpedi.jamanetwork.com/ by a University of California - San Francisco User on 03/20/2015
Insulin in Pediatric Diabetic Ketoacidosis Original Investigation Research
eter range were counterchecked by serum BG measurement
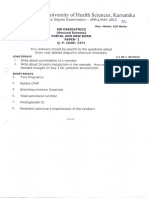
Figure 1. Trial Flow
using the hexokinase method. Serum electrolytes, urea, cre-
atinine, urine ketones, and venous blood gas were measured 57 Screened for eligibility
every 4 hours. Fluid intake, urine output, and electrocardio-
gram changes were monitored continuously, whereas neuro- 7 Excluded
logic assessment was performed every 2 hours. Malnutrition 5 Based on criteria decided
a priori
was defined based on weight for age matched for Indian 2 Cerebral edema at
standards.16 presentation
1 Received prereferral insulin
2 Septic shock with
Treatment Failure prereferral fluids
2 Excluded because of
The data were reviewed every 4 hours in both groups. Failure other reasons
to achieve a BG reduction of 18 mg/dL per hour for 2 consecu- 1 Suspected IEM
1 Missed
tive hours and/or a decrease or failure to increase in bicarbon-
ate with persistent high anion gap acidosis was considered a
50 Enrolled
nonresponse. A careful review of insulin therapy was per-
formed for errors in dose, preparation, or infusion rate before
labeling the nonresponse as treatment failure. The existing in- Randomization
fusion rate was thereafter increased by 0.02 U/kg per hour.
25 Allocated to low-dose 25 Allocated to standard-
Outcome Measures group dose group
The primary outcome was the rate of decrease in BG until the 25 Received allocated 25 Received allocated
intervention intervention
level reached 250 mg/dL or less. Time to resolution of acido-
sis, episodes of treatment failures, and incidences of hypoka-
0 Discontinued intervention 0 Discontinued intervention
lemia and hypoglycemia were secondary outcomes. Hypoka- 0 Lost to follow-up 0 Lost to follow-up
lemia was defined as a serum potassium level less than 3.5
mEq/L and/or suggestive electrocardiographic changes. 6
25 Analyzed 25 Analyzed
Hypoglycemia was defined as a BG level of 60 mg/dL or less. 0 Excluded from analysis 0 Excluded from analysis
Statistical Analysis IEM indicates inborn error of metabolism.
We estimated sample size to detect noninferiority; low dose
was considered noninferior if the difference between the stan-
dard and low dose for mean BG decrease did not exceed 18
mg/dL per hour. Previous data suggest that the SD of BG de- Results
crease with standard-dose insulin was 24 mg/dL per hour.17 Cal-
culated sample size with a power of 80% using a significance Baseline Characteristics
level of .05 (α = .05) was 44. Assuming an attrition rate of 10%, Figure 1 shows the trial profile. Of the 57 children screened for
we enrolled 50 participants in total. eligibility, 50 were enrolled and randomly assigned to the low-
Intergroup comparisons were performed using the t test dose (n = 25) or standard-dose (n = 25) group. Baseline demo-
and χ2 test with the Fisher exact test. For assessment of non- graphic and biochemical characteristics in both groups were
inferiority, we calculated the differences in BG decrease be- well matched (Table 1). A total of 13 children (26%) were
tween the 2 groups with 95% CIs and compared the upper limit younger than 5 years. New-onset diabetes presenting as DKA
of the CI to the preset noninferiority margin. To mitigate the was seen in 29 children (58%). A total of 34 children (68%) had
problem of multiple testing for serially measured quantita- severe DKA (pH <7.1 or bicarbonate <5 mEq/L). Twenty-six chil-
tive outcomes, we used repeated-measures analysis of vari- dren (52%) presented with hypoperfusion that required fluid
ance and a summary measure of areas under the curve. To es- bolus in the first hour. The mean BG decrease after the first hour
timate the area under the curve from baseline until 6 hours of of fluid therapy was 65 mg/dL (range, 12-190 mg/dL). Inci-
insulin therapy, we imputed missing values (few participants dence of mechanical problems encountered during fluid and
in whom target BG values were attained before 6 hours) with insulin infusions were similar in the low- and standard-dose
multivariate imputation by chained equations. groups (2 vs 4 mechanical problems).
Hazard ratios (HRs) were estimated for outcomes of BG de-
crease and resolution of acidosis using Cox proportional model BG Decrease
adjusted a priori for age, weight, and acidosis severity. For all The mean (SD) rate of BG decrease per hour until the level was
secondary outcomes, the Monte Carlo permutation test was 250 mg/dL or less was similar in the groups (45.1 [17.6] vs
performed to adjust for multiple outcomes. For primary out- 52.2 [23.4] in the low-dose vs standard-dose group). The dif-
come, P < .05 was considered statistically significant. Data en- ference in mean rates was 7.2 mg/dL per hour (95% CI, −4.7 [fa-
try and analysis were performed using IBM-SPSS, version 22 voring low dose] to 19 [favoring standard dose] mg/dL per hour;
(SPSS Inc), MedCalc, version 13.2 (MedCalc Software), and Stata/ the upper limit of the 95% CI just barely surpassing the a priori
IC, version 12 (Stata Corp). noninferiority margin of 18 mg/dL per hour) (Table 2). The mean
jamapediatrics.com JAMA Pediatrics November 2014 Volume 168, Number 11 1001
Copyright 2014 American Medical Association. All rights reserved.
Downloaded From: http://archpedi.jamanetwork.com/ by a University of California - San Francisco User on 03/20/2015
Research Original Investigation Insulin in Pediatric Diabetic Ketoacidosis
dard- compared with low-dose insulin (61 vs 39 mg/dL) (Table 2).
Table 1. Baseline Demographic and Biochemical Characteristicsa
Episodes of BG decrease greater than the desired range (>90 mg/
Low-Dose Standard-Dose dL) were also more frequent with the former compared with the
Group Group
Characteristic (n = 25) (n = 25) latter (12 [10%] of 124 vs 4 [4%] of 113; relative risk, 0.51; 95%
Age, mean (SD), y 7.3 (3.8) 6.5 (3.6) CI, 0.21-1.20; P = .05). In fact, no out-of-range decrease was noted
Sex with low-dose insulin during the first hour of infusion.
Male 9 (36) 11 (44) No difference was found in the mean (SD) length of time
Female 16 (64) 14 (56) to achieve a BG level of 250 mg/dL or less between low- and
Weight at admission, mean (SD), kg 19.2 (9.1) 17.3 (7.3) standard-dose groups (6.0 [3.3] vs 6.2 [2.2] hours; P = .80). Sev-
Weight after DKA correction, 19.5 (9.1) 18.0 (7.4) enteen children in the low-dose group and 15 in the standard-
mean (SD), kg dose group attained the BG target (≤250 mg/dL) by 6 hours
Children with malnutrition 7 (28) 8 (32) (Figure 2). The HR of achieving a BG level of 250 mg/dL or less
New-onset DKA 13 (52) 16 (64) by the end of 6 hours was 1.32 times higher in the low-dose
Established diabetes mellitus 12 (48) 9 (36) group compared with the standard-dose group (adjusted HR,
Duration of diabetes, mean (SD), mo 23.5 (25.2) 18.6 (13.2) 1.32; 95% CI, 0.64-2.73). However, this difference was not sta-
Children with previous DKA 6 (50) 6 (67) tistically significant (P = .45) (eFigure 1 in the Supplement).
Hemodynamic status at admission
Compensated shock 12 (48) 13 (52) Resolution of Acidosis
Hypotensive shock 1 (4) 0 The mean (SD) length of time for resolution of acidosis (end
GCS score of 12-14 at admission 6 (24) 9 (36) point) was 16.5 (7.2) hours in the low-dose group and 17.2
Blood glucose, mean (SD), mg/dL 485.3 (133) 524.4 (103) (7.7) hours in the standard-dose group (P = .73) (Table 3). The
pH, mean (SD) 7.08 (0.12) 7.05 (0.11) rate of resolution of acidosis and serial changes in pH, bicar-
Bicarbonate, mean (SD), mEq/L 6.2 (2.6) 7.0 (3.1) bonate, and anion gap were all similar (Figure 3). The HR of
Anion gap, mean (SD) 27.5 (4.9) 28.0 (8.5) resolution of acidosis by 24 hours was lower by 22% in the low-
PCO2, mean (SD), mm Hg 19.4 (4.9) 23.0 (7.7)
dose group compared with the standard-dose group (ad-
justed HR, 0.78; 95% CI, 0.41-1.47). This difference was not sta-
Urea, mean (SD), mg/dL 34.1 (9.7) 39.4 (16.3)
tistically significant (P = .44) (eFigure 2 in the Supplement).
Creatinine, mean (SD), mg/dL 0.7 (0.3) 0.7 (0.2)
Sodium, mean (SD), mEq/L 133.0 (7.0) 134.5 (10.0)
Therapy-Related Complications
Corrected sodium, mean (SD), mEq/L 138.9 (6.7) 141.3 (10.3)
Twelve children (48%) in the standard-dose group compared
Effective osmolality, 292.0 (13.8) 298.2 (21.2)
mean (SD), mOsm/kg with 5 (20%) in the low-dose group had at least one episode of
Potassium, mean (SD), mEq/L 4.8 (0.8) 4.7 (0.7) hypokalemia (P = .07). This tendency was more pronounced in
Phosphorus, mean (SD), mg/dL 3.0 (1.1) 2.9 (1.0) malnourished children (7 [88%] in the standard-dose group vs
Urine ketones 2 [28%] in the low-dose group) (eTable in the Supplement). Epi-
4+ (>160 mg/dL) 20 (80) 17 (68) sodes of hypoglycemia were also higher with the standard dose,
3+ (80-160 mg/dL) 5 (20) 8 (32) but the difference did not reach statistical significance (5 [20%]
Fluid received before 12.7 (7.3) 12.7 (7.7)
vs 1 [4%] in the standard-dose group vs low-dose group; P = .17).
starting insulin, More children required measures to counter decreasing BG lev-
mean (SD), mL/kg
els (dextrose increments to ≥10%) in the standard-dose group
Blood glucose decrease with initial 65.1 (32.8) 65.2 (41.4)
hour of hydration before starting insulin, (7 [28%] vs 2 [8%] in the standard-dose group vs low-dose group;
mean (SD), mg/dL P = .14) (Table 3). One child in the standard-dose group re-
Duration of 0.9% saline therapy, 6.6 (1.9) 7.0 (1.9) quired insulin dose reduction to 0.08 U/kg per hour because of
mean (SD), h
persistent BG levels less than 100 mg/dL despite 12.5% dex-
Abbreviations: DKA, diabetic ketoacidosis; GCS, Glasgow Coma Scale.
trose infusion. Two children (8%) in the low-dose group and 1
SI conversion factors: To convert glucose to millimoles per liter, multiply by
(4%) in the standard-dose group had treatment failure. Both chil-
0.0555; to convert bicarbonate, sodium, and potassium to millimoles per liter,
multiply by 1; to convert urea to millimoles per liter, multiply by 0.17; to convert dren in the former group had new-onset diabetes with severe
creatinine to micromoles per liter, multiply by 88.4; and to convert phosphorus DKA that required increment in insulin to 0.07 U/kg per hour
to millimoles per liter, multiply by 0.323. at 8 and 12 hours of therapy, respectively. However, no further
a
Data are presented as number (percentage) of children unless otherwise increments were needed until the resolution of acidosis. Only
indicated.
one child in the study cohort developed cerebral edema (stan-
dard-dose group). No deaths occurred in either treatment group
area under the curve values were also similar (AUC, 2201; 95% during the study period.
CI, 2014-2388; vs AUC, 2263; 95% CI, 2093-2434; for low dose
vs standard dose; t = 0.49; P = .62).
The serial (hourly) changes in rate of decrease and percent-
age decrease in BG between the groups revealed no significant
Discussion
difference (F = 0.47; P = .71). However, the mean decrease in BG We found that the BG reduction achieved with low-dose insu-
at the end of first hour of insulin infusion was higher with stan- lin was noninferior to that achieved with standard-dose insu-
1002 JAMA Pediatrics November 2014 Volume 168, Number 11 jamapediatrics.com
Copyright 2014 American Medical Association. All rights reserved.
Downloaded From: http://archpedi.jamanetwork.com/ by a University of California - San Francisco User on 03/20/2015
Insulin in Pediatric Diabetic Ketoacidosis Original Investigation Research
Table 2. Primary Outcome Measures (Blood Glucose Decrease)a
Low-Dose Standard-Dose Difference
Group Group Between Means
Measure (n = 25) (n = 25) (95% CI)
Mean blood glucose decrease until level 45.1 (17.6) 52.2 (23.4) –7.2 (–19 to 4.7)
is ≤250 mg/dL, mg/dL per hour
Blood glucose decrease, mg/dL per hour
0-1 h 39.2 (25.5) 61.3 (37.7) –21.6 (–39.8 to –3.2)
1-2 h 48.6 (37.7) 39.6 (28.8) 9 (–10 to 28.1)
2-3 h 54.0 (34.2) 37.7(32.4) 16.2 (–2.7 to 35.1)
3-4 h 37.7 (39.6) 41.4 (39.6) –3.6 (–26.1 to 18.9)
Blood glucose decrease, %
0-1 h 9.3 (6.4) 13.8 (8.3) –4.5 (–8.71 to –0.28)
0-2 h 19.3 (10.4) 22.2 (10.9) –2.9 (–8.95 to 3.15)
0-3 h 28.4 (10.6) 26.7 (8.8) 1.7 (–3.84 to 7.24)
0-4 h 33.8 (11.0) 34.6 (13.8) –0.8 (–7.89 to 6.29)
Time taken to achieve blood glucose level 6.0 (3.3) 6.2 (2.2) 0.79 (–1.79 to 1.39)
of ≤250 mg/dL, h
Absolute blood glucose decrease until 209 (112) 239 (111) –30 (–93.41 to 33.41)
level is ≤250 mg/dL, mg/dL a
Data are presented as mean (SD).
Table 3. Secondary Outcome Measuresa
Low-Dose Standard-Dose
Group Group
Measure (n = 25) (n = 25) P Value
Time until resolution of acidosis, mean (SD), h 16.5 (7.2) 17.2 (7.7) .73
Children with hypokalemia 5 (20) 12 (48) .07b
Children with hypoglycemia 1 (4) 5 (20) .17b a
Data are presented as number
Children requiring dextrose concentration ≥10% 2 (8) 7 (28) .14b (percentage) of children unless
otherwise indicated.
Treatment failure 2 (8) 1 (4)
b
P value by Monte Carlo permutation
Cerebral edema 0 1 (4)
test.
lin, although the overall reduction with both regimens re- electrolytes, thus increasing the risk of cerebral edema.13 Most
mained within the reported range (36-90 mg/dL). The decrease guidelines, therefore, have eliminated first-hour insulin be-
in BG during insulin therapy is the cumulative effect of sup- cause hydration alone has been reported to cause a mean BG
pression of hepatic glucose production, stimulation of periph- decrease of 109 mg/dL by improving renal perfusion and clear-
eral glucose uptake, and renal glycosuria, with the first action ing osmolar load.11
being the most important.2 However, patients with DKA ex- Our situation is compounded by delayed presentation,
hibit some degree of hepatic resistance to insulin action, ne- missed or delayed diagnosis, and lack of optimum therapy in
cessitating higher plasma insulin levels (80-100 μU/mL) to off- those diagnosed as having DKA before referral.20 These chil-
set this resistance,18 meaning that any effective dose of insulin dren tend to be severely acidotic and hyperosmolar, thus mak-
in DKA should achieve these levels. On the contrary, the cur- ing the initial hours of therapy more cautious and geared to-
rently recommended standard dose of 0.1 U/kg per hour has been ward prevention of osmotic disequilibrium. 14 In light of
reported to achieve a plasma insulin concentration much higher previously reported observations that confirm that severity of
than the optimal requisite range (100-200 μU/mL).4,19 This is the baseline biochemical abnormalities coupled with early insu-
justification given in some studies9,10 for lowering the insulin lin and large volumes of fluid increase the risk of cerebral
dose to achieve the desired therapeutic response with mini- edema,13 our observations on the differences in rate of BG de-
mal adverse effects. Although we did not measure plasma in- crease between low and standard doses of insulin in the ini-
sulin levels in this study, our findings extend the above postu- tial hours could be of interest. We found more episodes of out-
late prospectively to show that low-dose insulin achieves a of-range (>90 mg/dL) BG decreases with standard-dose insulin.
clinically effective BG reduction comparable to standard dose. On the contrary, the rate of decrease with low-dose insulin in-
Initial hours of DKA management are a matter of concern creased gradually every hour until 3 hours to achieve a maxi-
and controversy. Increasing evidence indicates that fluids and mum decrease (54 mg/dL). This finding suggests that the lower
insulin have to be used cautiously in the early hours to pre- dose may be a safer option, particularly in situations in which
vent a precipitous decrease in BG, rapid electrolyte shifts, and a gradual decrease in glucose, electrolytes, and resultant os-
resultant osmotic disequilibrium.10-12 Evidence indicates that molality is desired.
higher insulin doses in the first few hours can aggravate a BG We found that low-dose insulin was not inferior to the stan-
decrease but more importantly may lead to rapid changes in dard dose in correcting acidosis. The time to resolution of aci-
jamapediatrics.com JAMA Pediatrics November 2014 Volume 168, Number 11 1003
Copyright 2014 American Medical Association. All rights reserved.
Downloaded From: http://archpedi.jamanetwork.com/ by a University of California - San Francisco User on 03/20/2015
Research Original Investigation Insulin in Pediatric Diabetic Ketoacidosis
Figure 2. Mean Blood Glucose Decrease With Insulin Therapy Figure 3. Mean Serial Changes in pH, Bicarbonate, and Anion Gap
600 7.40
Low dose Low dose
Standard dose 7.35 Standard dose
(7) (6)
(14)
550 7.30 (21)
(25) (6)
7.25 (11)
500 (21) (15)
7.20 (25)
pH
(25)
(24)
7.15
Blood Glucose, mg/dL
450 (25)
7.10
(25) (25)
400 7.05
(25)
(25) (25) 7.00
(24) (21)
350 6.95
(22) (18) (8)
(13) 0 4 8 12 16 20 24
(19) Duration of Therapy, h
300
(16)
(10) 17
(16)
250
15
(6)
(21) (14)
Bicarbonate, mEq/L
13 (11)
200
0 1 2 3 4 5 6 (25)
Duration of Insulin Therapy, h 11 (15)
(21) (7) (6)
9 (25)
The numbers of children who had not attained a blood glucose level of (25)
(24)
250 mg/dL or less at each hour are given in parentheses (P = .71, F = 0.47 for the 7
difference between the 2 groups). To convert blood glucose values to millimoles (25) (25)
5
per liter, multiply by 0.0555. Error bars indicate SD.
3
0 4 8 12 16 20 24
Duration of Therapy, h
dosis was similar in both, suggesting that the low dose could
be as effective as the standard dose in suppressing lipolysis and 35
ketogenesis. Episodes of treatment failures were also rare, and 30 (25)
few patients required incremental insulin while on the low- 25
(25)
(25) (24)
dose regimen. Two studies9,10 that compared the 2 insulin regi- (21) (7)
Anion Gap
20 (25) (14) (6)
mens have reported similar efficacy in both. Although these
15 (25) (21)
studies concur with the findings reported by us, they differ (15)
(11)
from our study on 2 accounts. Both studies are retrospective 10
(6)
and the duration was shorter than the usual described dura- 5
tion of reversal of DKA. 0
Hypokalemia has remained the most frequent complica- 0 4 8 12 16 20 24
Duration of Therapy, h
tion of DKA in our setup, with the reported incidence varying
from 41% to 82%, much higher than the 4% to 10% reported
The numbers of children who had not attained end point at each measurement
by our Western counterparts.14,17,21 Underlying malnutrition, are given in parentheses (P = .82, F = 0.36; P = .53, F = 0.77; and P = .15, F = 1.9
poor total body stores of potassium, prolonged illness before for the difference between the 2 groups in pH, bicarbonate, and anion gap,
presentation, and osmotic diuresis are some of the causal fac- respectively). Error bars indicate SD.
tors for hypokalemia in our patients. In this study too, hypo-
kalemia emerged as the most frequent complication (34%). In speculate that low-dose insulin will be a safer option as far as
addition to these factors, the dose of insulin could have also therapy-related complications of DKA are concerned.
played a role in lowering serum potassium levels because there Our study has several strengths. First, to the best of our
was a trend toward a higher proportion of hypokalemia in stan- knowledge, this is the first prospective experiment compar-
dard- compared with low-dose insulin. Likewise, hypoglyce- ing the 2 insulin regimens with a sizeable sample. Second, un-
mia is another important therapy-related complication aggra- like other studies,9,10 our patients have been followed up un-
vated by associated malnutrition in our setting. A study by til the resolution of acidosis. We also have looked at factors
Moulik et al17 reported the incidence to be 30.3% with standard- unique to developing economies, thus making the applicabil-
dose insulin, which increased to 64% when malnourished chil- ity of our results more tenable to similar conditions. We be-
dren alone were considered. In the current study, the inci- lieve the limitations associated with an open-label study de-
dence of hypoglycemia was, however, lower (12%). Although sign were minimized by the objective nature of our study
stringent BG monitoring could have contributed to this de- outcomes. However, a few limitations need mention. We could
creased incidence, the effect of low-dose insulin cannot be not enroll adolescent children with DKA because our unit ca-
completely negated. On the basis of our results, we strongly ters only to children 12 years or younger. A noninferiority mar-
1004 JAMA Pediatrics November 2014 Volume 168, Number 11 jamapediatrics.com
Copyright 2014 American Medical Association. All rights reserved.
Downloaded From: http://archpedi.jamanetwork.com/ by a University of California - San Francisco User on 03/20/2015
Insulin in Pediatric Diabetic Ketoacidosis Original Investigation Research
gin of 18 mg/dL per hour selected in our trial was possibly strin-
gent. Although the upper limit of the 95% CI for mean Conclusion
difference (19 mg/dL) just exceeded the noninferiority mar-
gin, it was less than the entire assumed treatment effect and Low-dose insulin is noninferior to standard-dose insulin with
hence is a statistically persuasive finding. In a clinical con- respect to the rate of BG decrease and resolution of acidosis.
text too, an inferior BG decrease when associated with con- Our study opens the door for a subsequent trial with a larger
tinuing resolution of acidosis is acceptable. Nonetheless, a su- sample size to explore differences in the rate of BG decrease
periority trial with a larger sample size could possibly have before 0.05 U/kg per hour replaces 0.1 U/kg per hour in the prac-
brought out differences in the primary outcome. tice recommendations.
ARTICLE INFORMATION 4. Kitabchi AE, Ayyagari V, Guerra SM. The efficacy glucose-corrected serum sodium and neurological
Accepted for Publication: June 3, 2014. of low-dose versus conventional therapy of insulin status in severe diabetic ketoacidosis. Arch Dis Child.
for treatment of diabetic ketoacidosis. Ann Intern 2011;96(1):50-57.
Published Online: September 29, 2014. Med. 1976;84(6):633-638.
doi:10.1001/jamapediatrics.2014.1211. 13. Edge JA, Jakes RW, Roy Y, et al. The UK
5. Burghen GA, Etteldorf JN, Fisher JN, Kitabchi case-control study of cerebral oedema complicating
Author Contributions: Dr Jayashree had full access AQ. Comparison of high-dose and low-dose insulin diabetic ketoacidosis in children. Diabetologia.
to all the data in the study and takes responsibility by continuous intravenous infusion in the 2006;49(9):2002-2009.
for the integrity of the data and the accuracy of the treatment of diabetic ketoacidosis in children.
data analysis. 14. Jayashree M, Singhi S. Diabetic ketoacidosis:
Diabetes Care. 1980;3(1):15-20. predictors of outcome in a pediatric intensive care
Study concept and design: All authors.
Acquisition, analysis, or interpretation of data: 6. Dunger DB, Sperling MA, Acerini CL, et al; ESPE; unit of a developing country. Pediatr Crit Care Med.
Nallasamy. LWPES. ESPE/LWPES consensus statement on 2004;5(5):427-433.
Drafting of the manuscript: Nallasamy, Jayashree, diabetic ketoacidosis in children and adolescents. 15. Variable block randomization software.
Bansal. Arch Dis Child. 2004;89(2):188-194. http://randomization.com. Accessed July 1, 2011.
Critical revision of the manuscript for important 7. Wolfsdorf J, Craig ME, Daneman D, et al. Diabetic 16. Nutrition Sub-Committee of the Indian
intellectual content: Jayashree, Singhi. ketoacidosis in children and adolescents with Academy of Pediatrics. Report of Convener. Indian
Statistical analysis: Nallasamy, Jayashree. diabetes. Pediatr Diabetes. 2009;10(suppl 12):118- Pediatr. 1972;9:360.
Administrative, technical, or material support: 133.
Jayashree, Singhi, Bansal. 17. Moulik NR, Jayashree M, Singhi S, Bhalla AK,
8. Noyes KJ, Crofton P, Bath LE, et al. Attri S. Nutritional status and complications in
Study supervision: Singhi, Bansal. Hydroxybutyrate near-patient testing to evaluate a children with diabetic ketoacidosis. Pediatr Crit
Conflict of Interest Disclosures: None reported. new end-point for intravenous insulin therapy in Care Med. 2012;13(4):e227-e233.
Additional Contributions: Sahul Bharti, MD (Build the treatment of diabetic ketoacidosis in children.
Pediatr Diabetes. 2007;8(3):150-156. 18. DeFronzo RA, Hendler R, Simonson D. Insulin
Healthy India Movement), provided assistance in resistance is a prominent feature of
statistical analysis. He did not receive any 9. Puttha R, Cooke D, Subbarayan A, et al; North insulin-dependent diabetes. Diabetes. 1982;31(9):
compensation for his contributions. West England Paediatric Diabetes Network. Low 795-801.
dose (0.05 units/kg/h) is comparable with standard
REFERENCES dose (0.1 units/kg/h) intravenous insulin infusion 19. Soler NG, FitzGerald MG, Wright AD, Malins JM.
for the initial treatment of diabetic ketoacidosis in Comparative study of different insulin regimens in
1. Umpierrez GE, Khajavi M, Kitabchi AE. Review: management of diabetic ketoacidosis. Lancet. 1975;
diabetic ketoacidosis and hyperglycemic children with type 1 diabetes—an observational
study. Pediatr Diabetes. 2010;11(1):12-17. 2(7947):1221-1224.
hyperosmolar nonketotic syndrome. Am J Med Sci.
1996;311(5):225-233. 10. Al Hanshi S, Shann F. Insulin infused at 0.05 20. Jayashree M, Rohit S, Singhi S. Root cause
versus 0.1 units/kg/hr in children admitted to analysis of diabetic ketoacidosis and its
2. Luzi L, Barrett EJ, Groop LC, Ferrannini E, complications: a developing country experience.
DeFronzo RA. Metabolic effects of low-dose insulin intensive care with diabetic ketoacidosis. Pediatr
Crit Care Med. 2011;12(2):137-140. Intensive Care Med. 2013;39(suppl 2):S242.
therapy on glucose metabolism in diabetic
ketoacidosis. Diabetes. 1988;37(11):1470-1477. 11. Bradley P, Tobias JD. Serum glucose changes 21. Kitabchi AE, Umpierrez GE, Murphy MB, et al.
during insulin therapy in pediatric patients with Management of hyperglycemic crises in patients
3. Alberti KGMM, Hockaday TDR, Turner RC. Small with diabetes. Diabetes Care. 2001;24(1):131-153.
doses of intramuscular insulin in the treatment of diabetic ketoacidosis. Am J Ther. 2007;14(3):265-268.
diabetic “coma.” Lancet. 1973;2(7828):515-522. 12. Durward A, Ferguson LP, Taylor D, Murdoch IA,
Tibby SM. The temporal relationship between
jamapediatrics.com JAMA Pediatrics November 2014 Volume 168, Number 11 1005
Copyright 2014 American Medical Association. All rights reserved.
Downloaded From: http://archpedi.jamanetwork.com/ by a University of California - San Francisco User on 03/20/2015
S-ar putea să vă placă și
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5795)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- Patent Ductus Arteriosus 2014Document10 paginiPatent Ductus Arteriosus 2014Neha OberoiÎncă nu există evaluări
- Cardiomyopathy CircDocument20 paginiCardiomyopathy CircNeha OberoiÎncă nu există evaluări
- Neonatology Guidelines NHS PDFDocument364 paginiNeonatology Guidelines NHS PDFNeha OberoiÎncă nu există evaluări
- TTTS NeoreviewsDocument13 paginiTTTS NeoreviewsNeha OberoiÎncă nu există evaluări
- Qpaper Rguhs Pediatrics April May 2015Document4 paginiQpaper Rguhs Pediatrics April May 2015Neha OberoiÎncă nu există evaluări
- Agyria-PachygyriaDocument6 paginiAgyria-PachygyriaNeha OberoiÎncă nu există evaluări
- Letters and Correspondence: American Journal of Hematology 75:115-120 (2004)Document6 paginiLetters and Correspondence: American Journal of Hematology 75:115-120 (2004)Neha OberoiÎncă nu există evaluări
- Neonatal TransportDocument19 paginiNeonatal TransportNeha OberoiÎncă nu există evaluări
- Clinical and Etiological Profile of Acute Febrile Encephalopathy in Eastern NepalDocument3 paginiClinical and Etiological Profile of Acute Febrile Encephalopathy in Eastern NepalNeha OberoiÎncă nu există evaluări
- Pedsap 1 ImmunologyDocument96 paginiPedsap 1 ImmunologyNeha Oberoi100% (1)
- Amateur TransplantsDocument5 paginiAmateur TransplantsNeha OberoiÎncă nu există evaluări
- Paediatrics PDFDocument44 paginiPaediatrics PDFNeha OberoiÎncă nu există evaluări
- PediatricsDocument48 paginiPediatricsNeha OberoiÎncă nu există evaluări
- 1 Al 2012Document1 pagină1 Al 2012Neha OberoiÎncă nu există evaluări
- Guidelines & InstructionsDocument2 paginiGuidelines & InstructionsNeha OberoiÎncă nu există evaluări
- Enhancing Case Detection of Selected Inherited Disorders Through Expanded Newborn Screening in The PhilippinesDocument7 paginiEnhancing Case Detection of Selected Inherited Disorders Through Expanded Newborn Screening in The PhilippinesDerekBryanÎncă nu există evaluări
- Case Study Chronic CholecystitisDocument24 paginiCase Study Chronic CholecystitisShehada Marcos BondadÎncă nu există evaluări
- MR in Neuro: Clinical Work and Research by Our UsersDocument48 paginiMR in Neuro: Clinical Work and Research by Our UsersJose luis EspinosaÎncă nu există evaluări
- Conjunctiva Anatomy and PhysiologyDocument101 paginiConjunctiva Anatomy and PhysiologyPurva KeswaniÎncă nu există evaluări
- Health Implication and Complication of Herbal MedicineDocument26 paginiHealth Implication and Complication of Herbal Medicineigweonyia gabrielÎncă nu există evaluări
- Pressure Ulcer Prevention Master ClassDocument8 paginiPressure Ulcer Prevention Master ClassmirantikaÎncă nu există evaluări
- Homework Lecture - Vitamin DDocument6 paginiHomework Lecture - Vitamin DJoana TolentinoÎncă nu există evaluări
- ICD For OncologyDocument337 paginiICD For OncologytphivuongÎncă nu există evaluări
- Antiepileptic Drugs: Presenter: DR Sanjeev Sharma Guide: DR Komal PrasadDocument50 paginiAntiepileptic Drugs: Presenter: DR Sanjeev Sharma Guide: DR Komal PrasadSanjeev SharmaÎncă nu există evaluări
- PneumothoraxDocument11 paginiPneumothoraxManoj RanadiveÎncă nu există evaluări
- 2007 Electrocardiographic Manifestations Pediatric EcgDocument10 pagini2007 Electrocardiographic Manifestations Pediatric EcgAngel NspÎncă nu există evaluări
- PNLE III Nursing PracticeDocument11 paginiPNLE III Nursing PracticeASDF ASDFÎncă nu există evaluări
- DR Abdul Kalam - President of India Speech at Medical ConferenceDocument7 paginiDR Abdul Kalam - President of India Speech at Medical ConferenceSibia SukhbindarÎncă nu există evaluări
- List of Common Drugs-UpdatedDocument29 paginiList of Common Drugs-UpdatedPaul Benjomin AgregadoÎncă nu există evaluări
- Liver Cirrhosis: Etiology Pathogenesis Clinical Features Management PrognosisDocument35 paginiLiver Cirrhosis: Etiology Pathogenesis Clinical Features Management PrognosisMohd Johari Mohd ShafuwanÎncă nu există evaluări
- The ST Kitts Eye StudyDocument50 paginiThe ST Kitts Eye StudyPaul H ArtesÎncă nu există evaluări
- Presentor: DR - Kumar Moderator: DR - VamsidharDocument71 paginiPresentor: DR - Kumar Moderator: DR - VamsidharJayaprakash KuppusamyÎncă nu există evaluări
- 3Document26 pagini3Andreea100% (1)
- Amyloidosis: Marwa Bawab - SP 10Document51 paginiAmyloidosis: Marwa Bawab - SP 10Marrouch Ba100% (1)
- Obstetrics & Gynecology 2019 Bases Krok 2 Explaned - Students AssistantDocument157 paginiObstetrics & Gynecology 2019 Bases Krok 2 Explaned - Students AssistantAbhinav VermaÎncă nu există evaluări
- Tuberculosis in Children: Screening, Diagnosis and ManagementDocument10 paginiTuberculosis in Children: Screening, Diagnosis and ManagementSatria Bayu PratamaÎncă nu există evaluări
- The Colleges of Medicine of South AfricaDocument4 paginiThe Colleges of Medicine of South AfricaJustine NyangaresiÎncă nu există evaluări
- Microbial Diseases of The Skin & EyesDocument52 paginiMicrobial Diseases of The Skin & EyesAna100% (3)
- Relationships Among Concha Bullosa, Nasal Septal Deviation, and Sinusitis: Retrospective Analysis of 296 CasesDocument5 paginiRelationships Among Concha Bullosa, Nasal Septal Deviation, and Sinusitis: Retrospective Analysis of 296 CasesandiniÎncă nu există evaluări
- Shaukat Khanum Memorial Cancer Hospital & Research Centre: Specimen Nature: Specimen SiteDocument3 paginiShaukat Khanum Memorial Cancer Hospital & Research Centre: Specimen Nature: Specimen Siteshahid.bhai877605Încă nu există evaluări
- Management of Monochorionic Twin PregnancyDocument2 paginiManagement of Monochorionic Twin PregnancyWira PutriÎncă nu există evaluări
- The Milk's in The OvenDocument36 paginiThe Milk's in The Ovenkarthikv_79Încă nu există evaluări
- MCQS ANS 03 Sol PDFDocument4 paginiMCQS ANS 03 Sol PDFSamir Rekha Mukund Joshi100% (1)
- Census August 8 - August 9, 2020Document6 paginiCensus August 8 - August 9, 2020Patrick JohnÎncă nu există evaluări
- Progressive Idiopathic Condylar Resorption - Three Case ReportsDocument14 paginiProgressive Idiopathic Condylar Resorption - Three Case ReportsCatalina Soler LioiÎncă nu există evaluări