S-ar putea să vă placă și
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (587)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (73)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (265)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (119)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- I. Specifikacija Opreme Sa Ugradnjom R.Br. Opis JM KomDocument4 paginiI. Specifikacija Opreme Sa Ugradnjom R.Br. Opis JM KomAleksandar VidakovicÎncă nu există evaluări
- India's 1991 Economic ReformsDocument5 paginiIndia's 1991 Economic ReformsLive AspireÎncă nu există evaluări
- Personality, Movie Preferences, and RecommendationsDocument2 paginiPersonality, Movie Preferences, and RecommendationsAA0809Încă nu există evaluări
- Admission Notice 2023-24Document2 paginiAdmission Notice 2023-24Galav PareekÎncă nu există evaluări
- 2004 Canon Bino BrochureDocument6 pagini2004 Canon Bino BrochureCraig ThompsonÎncă nu există evaluări
- Cases 39 45 PDFDocument11 paginiCases 39 45 PDFYvette Marie VillaverÎncă nu există evaluări
- Kamera Basler Aca2500-20gmDocument20 paginiKamera Basler Aca2500-20gmJan KubalaÎncă nu există evaluări
- Mechanical Function of The HeartDocument28 paginiMechanical Function of The HeartKarmilahNÎncă nu există evaluări
- Baella-Silva v. Hulsey, 454 F.3d 5, 1st Cir. (2006)Document9 paginiBaella-Silva v. Hulsey, 454 F.3d 5, 1st Cir. (2006)Scribd Government DocsÎncă nu există evaluări
- As 91435Document3 paginiAs 91435api-271057641Încă nu există evaluări
- Summary Refinery Sulfur Recovery ProjectsDocument8 paginiSummary Refinery Sulfur Recovery ProjectsAli MÎncă nu există evaluări
- The English Center Articulation AgreementDocument9 paginiThe English Center Articulation AgreementJose CabreraÎncă nu există evaluări
- Bylaw 16232 High Park RezoningDocument9 paginiBylaw 16232 High Park RezoningJamie_PostÎncă nu există evaluări
- Ôn tập và kiểm tra học kì Tiếng anh 6 ĐÁP ÁNDocument143 paginiÔn tập và kiểm tra học kì Tiếng anh 6 ĐÁP ÁNThùy TinaÎncă nu există evaluări
- Linear Circuit Analysis (ELEN-1100) : Lecture # 13: More On Mesh Current AnalysisDocument11 paginiLinear Circuit Analysis (ELEN-1100) : Lecture # 13: More On Mesh Current AnalysisPhD EEÎncă nu există evaluări
- Cursos Link 2Document3 paginiCursos Link 2Diego Alves100% (7)
- Mod. 34 Classic Compact T06Document4 paginiMod. 34 Classic Compact T06Jaime Li AliÎncă nu există evaluări
- Interviews: Personal Interview. Advantages and Disadvantages Business Is Largely A Social PhenomenonDocument8 paginiInterviews: Personal Interview. Advantages and Disadvantages Business Is Largely A Social PhenomenonSanjeev JayaratnaÎncă nu există evaluări
- The NicotinaDocument8 paginiThe Nicotinab0beiiiÎncă nu există evaluări
- VNACS Final Case ReportDocument9 paginiVNACS Final Case ReportVikram Singh TomarÎncă nu există evaluări
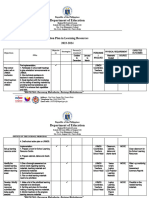
- aCTION PLAN IN HEALTHDocument13 paginiaCTION PLAN IN HEALTHCATHERINE FAJARDOÎncă nu există evaluări
- Affidavit of 2 Disinterested Persons (Haidee Gullodo)Document1 paginăAffidavit of 2 Disinterested Persons (Haidee Gullodo)GersonGamasÎncă nu există evaluări
- Mumbai Tourist Attractions.Document2 paginiMumbai Tourist Attractions.Guru SanÎncă nu există evaluări
- Chapter 27 Protists I. Evolution of EukaryotesDocument7 paginiChapter 27 Protists I. Evolution of EukaryotesNadeem IqbalÎncă nu există evaluări
- Building MassingDocument6 paginiBuilding MassingJohn AmirÎncă nu există evaluări
- XLVI ESAN INTERNATIONAL WEEK (MBA Only - July 2023)Document38 paginiXLVI ESAN INTERNATIONAL WEEK (MBA Only - July 2023)Juan Diego Fernández CastilloÎncă nu există evaluări
- Ground Floor 40X80 Option-1Document1 paginăGround Floor 40X80 Option-1Ashish SrivastavaÎncă nu există evaluări
- Me2404 Set1Document16 paginiMe2404 Set1sakthivelsvsÎncă nu există evaluări
- Rapid ECG Interpretation Skills ChallengeDocument91 paginiRapid ECG Interpretation Skills ChallengeMiguel LizarragaÎncă nu există evaluări
- Audit AP TestsDocument3 paginiAudit AP TestsSweet Emme100% (1)