S-ar putea să vă placă și
- Neurology Headache: Types and TreatmentDocument142 paginiNeurology Headache: Types and TreatmentMohammed Saad NabhanÎncă nu există evaluări
- AAA Recovery From Parkinsons FINALDocument422 paginiAAA Recovery From Parkinsons FINALmickelle100% (1)
- Mother's RemediesOver One Thousand Tried and Tested Remidies From Mothersof The United States and Canada by Ritter, Thomas Jefferson, 1855Document1.051 paginiMother's RemediesOver One Thousand Tried and Tested Remidies From Mothersof The United States and Canada by Ritter, Thomas Jefferson, 1855Gutenberg.org100% (2)
- Parkinson & Movement Disorder - PPT 1Document30 paginiParkinson & Movement Disorder - PPT 1Venosha GunasekaranÎncă nu există evaluări
- Parkinsons DiseaseDocument58 paginiParkinsons DiseasemuthuuÎncă nu există evaluări
- Cleft Lip and Palate Management: A Comprehensive AtlasDe la EverandCleft Lip and Palate Management: A Comprehensive AtlasRicardo D. BennunÎncă nu există evaluări
- Dysphagia Diagnosis 1and Treatment (Olle Ekberg) (Z-Lib - Org) (1) - 83-284Document202 paginiDysphagia Diagnosis 1and Treatment (Olle Ekberg) (Z-Lib - Org) (1) - 83-284Macarena Paz ÁlvarezÎncă nu există evaluări
- Surgery For Pharyngeal Pouch or Zekers DivertulaDocument19 paginiSurgery For Pharyngeal Pouch or Zekers DivertulaKumaran Bagavathi RagavanÎncă nu există evaluări
- Medical Surgical Nursin Answer KeyDocument22 paginiMedical Surgical Nursin Answer Keyicy43167% (3)
- Usg in CADocument3 paginiUsg in CAJasmine EffendiÎncă nu există evaluări
- Bilateral Nasolabial Cyst MarcoviceanuDocument4 paginiBilateral Nasolabial Cyst MarcoviceanubamsusiloÎncă nu există evaluări
- Bilateral Antrochoanal Polyps in an Adult Case ReportDocument3 paginiBilateral Antrochoanal Polyps in an Adult Case ReportCut Nanda FitriÎncă nu există evaluări
- Cleft Palate CaseDocument5 paginiCleft Palate CaseyomifÎncă nu există evaluări
- Laryngomalacia - PPTX Dr. FeriDocument114 paginiLaryngomalacia - PPTX Dr. FeriAldy BimaÎncă nu există evaluări
- Pleomorphic Multicentric Adenoma Submandibular GlandDocument3 paginiPleomorphic Multicentric Adenoma Submandibular GlandmawarmelatiÎncă nu există evaluări
- Bennett - 2011 - The Chelonian Respiratory SystemDocument15 paginiBennett - 2011 - The Chelonian Respiratory SystemdsouzapeixotoÎncă nu există evaluări
- A Thyroglossal Duct Cyst Causing Obstructive SleepDocument4 paginiA Thyroglossal Duct Cyst Causing Obstructive SleepChitaÎncă nu există evaluări
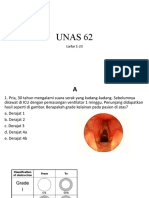
- UNAS 2022 Juni (Ke-62) Larfar 1-23, Al-Im 1-4Document51 paginiUNAS 2022 Juni (Ke-62) Larfar 1-23, Al-Im 1-4abubakar rizviÎncă nu există evaluări
- Supposed Otolaryngology Emergency Which Presents Late Bilateral Congenital Choanal AtresiaDocument3 paginiSupposed Otolaryngology Emergency Which Presents Late Bilateral Congenital Choanal AtresiaPaul HartingÎncă nu există evaluări
- Bedside Water Swallow Test ArticleDocument4 paginiBedside Water Swallow Test ArticleJU WSDÎncă nu există evaluări
- 2003 A Review of Surgical Treatment For Obstructive Sleep Apnoea Hypopnoea SyndromeDocument6 pagini2003 A Review of Surgical Treatment For Obstructive Sleep Apnoea Hypopnoea SyndromeRabia MekamchaÎncă nu există evaluări
- Lary 23467Document8 paginiLary 23467Dwi juliana DewiÎncă nu există evaluări
- Atrophic Rhinitis Slides 050330Document32 paginiAtrophic Rhinitis Slides 050330dan_srirahmadaniÎncă nu există evaluări
- A Huge Epiglottic Cyst Causing Airway Obstruction in An AdultDocument4 paginiA Huge Epiglottic Cyst Causing Airway Obstruction in An AdultWaleed KerÎncă nu există evaluări
- Surgical Approach to the Stylohyoid Process in Eagle’s SyndromeDocument3 paginiSurgical Approach to the Stylohyoid Process in Eagle’s SyndromekaluaxeniaÎncă nu există evaluări
- BJRCR 20150382Document3 paginiBJRCR 20150382Dewi Diana 龄龄Încă nu există evaluări
- Epiglottic Suture For Treatment of LaryngomalaciaDocument7 paginiEpiglottic Suture For Treatment of Laryngomalaciadr.hungsonÎncă nu există evaluări
- Article Thyroglose 1Document2 paginiArticle Thyroglose 1Jessica Paulina Salazar RuizÎncă nu există evaluări
- J Ijporl 2012 07 023Document3 paginiJ Ijporl 2012 07 023Nida Fariza MaulanisaÎncă nu există evaluări
- The Plunging Ranula Pathogenesis, Diagnosis and Management 1989Document4 paginiThe Plunging Ranula Pathogenesis, Diagnosis and Management 1989kaarlaamendezÎncă nu există evaluări
- Vocal Fold Polyp: Case ReportDocument9 paginiVocal Fold Polyp: Case ReportIndah Afriani NasutionÎncă nu există evaluări
- Congenital LaryngomalaciaDocument8 paginiCongenital LaryngomalaciaRettha SigiroÎncă nu există evaluări
- Airway ManagementDocument18 paginiAirway ManagementReza ManefoÎncă nu există evaluări
- Case Report Persistent Buccopharyngeal Membrane: Report of A Case and Review of The LiteratureDocument4 paginiCase Report Persistent Buccopharyngeal Membrane: Report of A Case and Review of The LiteratureLiviaÎncă nu există evaluări
- Laparoscopic Heller Myotomy For Achalasia: Robert N. Cacchione, M.D., Dan N. Tran, M.D., Diane H. Rhoden, M.DDocument5 paginiLaparoscopic Heller Myotomy For Achalasia: Robert N. Cacchione, M.D., Dan N. Tran, M.D., Diane H. Rhoden, M.Dgabriel martinezÎncă nu există evaluări
- Vocal Fold Scars - A Common Classifcation Proposal by The AmericanDocument4 paginiVocal Fold Scars - A Common Classifcation Proposal by The Americananitaabreu123Încă nu există evaluări
- Foreign Body Esophagus: When Endoscopic Removal FailsDocument3 paginiForeign Body Esophagus: When Endoscopic Removal FailsgheaastridgayatriÎncă nu există evaluări
- Tracheal StenosisDocument4 paginiTracheal StenosisJessica MarianoÎncă nu există evaluări
- Inner Ear Schwannoma - Publication by DR Tarek Khrais - Medics Index MemberDocument4 paginiInner Ear Schwannoma - Publication by DR Tarek Khrais - Medics Index MemberMedicsindex Telepin Slidecase100% (2)
- 495 FullDocument2 pagini495 Fulltigtigrai49Încă nu există evaluări
- Bab 2Document3 paginiBab 2Ratna WindyaningrumÎncă nu există evaluări
- Squamous Epithelial Changes of The Larynx: Diagnosis and TherapyDocument8 paginiSquamous Epithelial Changes of The Larynx: Diagnosis and TherapyIsrael BlancoÎncă nu există evaluări
- Paralisis Del HipoglosoDocument5 paginiParalisis Del HipoglosodrcesarpughÎncă nu există evaluări
- 1 s2.0 S1875459713001161 MainDocument4 pagini1 s2.0 S1875459713001161 Mainaieyha hamkaÎncă nu există evaluări
- Case Report: A Rare Cause of Upper Airway Obstruction in A ChildDocument4 paginiCase Report: A Rare Cause of Upper Airway Obstruction in A Childpagar bersihÎncă nu există evaluări
- Spiegel 2004Document5 paginiSpiegel 2004manuel abantoÎncă nu există evaluări
- Epiphrenic DiverticulumDocument1 paginăEpiphrenic DiverticulumInês PriorÎncă nu există evaluări
- Absesparafaring4 PDFDocument3 paginiAbsesparafaring4 PDFnataliayobeantoÎncă nu există evaluări
- Alexandria Workshop On Alexandria Workshop On Snoring & OSA SurgeryDocument17 paginiAlexandria Workshop On Alexandria Workshop On Snoring & OSA Surgeryrani suwadjiÎncă nu există evaluări
- The Uvulopalatal Flap in Soft Palate Reconstruction: Ahmad Zulkifli Ahmad Rashdi, Kelvin Lye Hock LimDocument5 paginiThe Uvulopalatal Flap in Soft Palate Reconstruction: Ahmad Zulkifli Ahmad Rashdi, Kelvin Lye Hock LimDrDejanDrakulÎncă nu există evaluări
- Aspiration: Definition: The Passage of Secretions Beyond The V.CDocument5 paginiAspiration: Definition: The Passage of Secretions Beyond The V.Cadham bani younesÎncă nu există evaluări
- Congenital Ankylosis of The Mandible: Report o F A Case N o T e D at BirthDocument3 paginiCongenital Ankylosis of The Mandible: Report o F A Case N o T e D at BirthRomzi HanifÎncă nu există evaluări
- LX Suspension and UES Myotomy Kos 2008Document7 paginiLX Suspension and UES Myotomy Kos 2008DEVÎncă nu există evaluări
- Clinical Review - Full PDFDocument6 paginiClinical Review - Full PDFDewi WulansariÎncă nu există evaluări
- Dr. Erjan Fikri, M. Ked. SPB, Spba (K)Document60 paginiDr. Erjan Fikri, M. Ked. SPB, Spba (K)ramadhan syah putraÎncă nu există evaluări
- Langmore 1988 Fiberoptic Endoscopic Examination of Swallowing SafetyDocument4 paginiLangmore 1988 Fiberoptic Endoscopic Examination of Swallowing SafetyDesiré MagalhãesÎncă nu există evaluări
- FELİNE-Upper Airway Obstruction in Cats Pathogenesis and Clinical SignsDocument7 paginiFELİNE-Upper Airway Obstruction in Cats Pathogenesis and Clinical Signstaner_soysuren100% (1)
- Bjorl: Congenital Laryngeal Saccular CystDocument1 paginăBjorl: Congenital Laryngeal Saccular CystGuilherme AméricoÎncă nu există evaluări
- Medi 96 E8514Document4 paginiMedi 96 E8514Syd BarretÎncă nu există evaluări
- Clasificacion ClinicaDocument3 paginiClasificacion ClinicaVillegas Valentín José AlbertoÎncă nu există evaluări
- Supraglottoplasty For Laryngomalacia PDFDocument7 paginiSupraglottoplasty For Laryngomalacia PDFVeronica GaticaÎncă nu există evaluări
- Quiz2 1 Issue2Document2 paginiQuiz2 1 Issue2Jazur AhamedÎncă nu există evaluări
- Urfer'S Ear: Exostoses of The External Auditory Canal: David B. Turetsky Fredericks. Vines, and David ClaymanDocument2 paginiUrfer'S Ear: Exostoses of The External Auditory Canal: David B. Turetsky Fredericks. Vines, and David Claymanprofesor conanÎncă nu există evaluări
- 401-Article Text-778-1-10-20190128 PDFDocument3 pagini401-Article Text-778-1-10-20190128 PDFCut Nanda FitriÎncă nu există evaluări
- The New Neurotology: A Comprehensive Clinical GuideDe la EverandThe New Neurotology: A Comprehensive Clinical GuideÎncă nu există evaluări
- Jco 18 01921Document24 paginiJco 18 01921mitaÎncă nu există evaluări
- Penting CI Zenner2016 PDFDocument13 paginiPenting CI Zenner2016 PDFmitaÎncă nu există evaluări
- Moran Jslpa 1989Document5 paginiMoran Jslpa 1989mitaÎncă nu există evaluări
- Oma La Copil PDFDocument11 paginiOma La Copil PDFmitaÎncă nu există evaluări
- Patfis Atik2011Document5 paginiPatfis Atik2011mitaÎncă nu există evaluări
- Prasad 2007Document5 paginiPrasad 2007mitaÎncă nu există evaluări
- Main Article PDFDocument17 paginiMain Article PDFmitaÎncă nu există evaluări
- Patfis Atik2011Document5 paginiPatfis Atik2011mitaÎncă nu există evaluări
- Bailey CH 161 Tinnitus and Hyperacusis-1-10Document10 paginiBailey CH 161 Tinnitus and Hyperacusis-1-10mitaÎncă nu există evaluări
- Tumor PDFDocument9 paginiTumor PDFmitaÎncă nu există evaluări
- Gradenigo Syndrome From Acute Sphenoiditis: A Case: OtolaryngologyDocument4 paginiGradenigo Syndrome From Acute Sphenoiditis: A Case: OtolaryngologymitaÎncă nu există evaluări
- Normal Heart Rate Ranges for Babies and ChildrenDocument7 paginiNormal Heart Rate Ranges for Babies and ChildrenmitaÎncă nu există evaluări
- Arch Dis Child 2016 Hilland 443 8Document7 paginiArch Dis Child 2016 Hilland 443 8mitaÎncă nu există evaluări
- Management of Gradenigo Syndrome in A ChildDocument4 paginiManagement of Gradenigo Syndrome in A ChildmitaÎncă nu există evaluări
- Otomycosis Case Report: Fungal Infection of the Ear CanalDocument24 paginiOtomycosis Case Report: Fungal Infection of the Ear CanalmitaÎncă nu există evaluări
- (Romanian Journal of Rhinology) Epistaxis Management - Our Point of View and Literature ReviewDocument7 pagini(Romanian Journal of Rhinology) Epistaxis Management - Our Point of View and Literature ReviewRizki AuditaÎncă nu există evaluări
- Adult Sinusitis Physicianresource Diagnostic Criteria RhinosinusitisDocument2 paginiAdult Sinusitis Physicianresource Diagnostic Criteria RhinosinusitismitaÎncă nu există evaluări
- Congenital Laryngeal WebsDocument3 paginiCongenital Laryngeal WebsmitaÎncă nu există evaluări
- Endoscopic Supraglottoplasty in Children With Severe Laryngomalacia With and Without Neurological ImpairmentDocument5 paginiEndoscopic Supraglottoplasty in Children With Severe Laryngomalacia With and Without Neurological ImpairmentmitaÎncă nu există evaluări
- Pa 1Document48 paginiPa 1mitaÎncă nu există evaluări
- S 1879729612000725Document7 paginiS 1879729612000725zzooooeeeeeeÎncă nu există evaluări
- Parotid Gland Tumor Case ReportDocument4 paginiParotid Gland Tumor Case ReportmitaÎncă nu există evaluări
- Understanding Sinusitis Diagnosis and TreatmentDocument15 paginiUnderstanding Sinusitis Diagnosis and TreatmentmitaÎncă nu există evaluări
- Pa 3Document87 paginiPa 3mitaÎncă nu există evaluări
- Case Report LMDocument2 paginiCase Report LMmitaÎncă nu există evaluări
- Epistaxis Anterior FinalDocument7 paginiEpistaxis Anterior FinalmitaÎncă nu există evaluări
- A Case of Giant Pleomorphic Adenoma of The Parotid GlandDocument3 paginiA Case of Giant Pleomorphic Adenoma of The Parotid GlandmitaÎncă nu există evaluări
- Management of Perichondritis of the AuricleDocument6 paginiManagement of Perichondritis of the AuriclemitaÎncă nu există evaluări
- Moran Jslpa 1989Document5 paginiMoran Jslpa 1989mitaÎncă nu există evaluări
- 1 s2.0 S1353802007002374 MainDocument10 pagini1 s2.0 S1353802007002374 MainBetty CastÎncă nu există evaluări
- Neurologist Communicationg The Diagnosis of ELADocument9 paginiNeurologist Communicationg The Diagnosis of ELAHabib G. Moutran BarrosoÎncă nu există evaluări
- Parkinson26 PDFDocument8 paginiParkinson26 PDFLorenaÎncă nu există evaluări
- Disorders of MovementDocument31 paginiDisorders of MovementNaghib BogereÎncă nu există evaluări
- IAS OUR DREAM NOTES COMPILATION PART 3 (17 - 23rd Nov.2013)Document45 paginiIAS OUR DREAM NOTES COMPILATION PART 3 (17 - 23rd Nov.2013)Swapnil Patil50% (2)
- Essay With FootnotesDocument7 paginiEssay With Footnotesafibafftauhxeh100% (2)
- Sifrol® ER: What Is in This LeafletDocument3 paginiSifrol® ER: What Is in This LeafletDenaraAshaPutriÎncă nu există evaluări
- 2001 Blum PIN PDFDocument38 pagini2001 Blum PIN PDFMasita Luthfi V PÎncă nu există evaluări
- HyeDounOctNovDec2010 PSDocument12 paginiHyeDounOctNovDec2010 PSanrcinfoÎncă nu există evaluări
- (Mohammadi 2022) 4D Printing of Soft Orthoses For Tremor SuppressionDocument22 pagini(Mohammadi 2022) 4D Printing of Soft Orthoses For Tremor SuppressionCarlos Gianpaul Rincón RuizÎncă nu există evaluări
- Timed Up and Go TestDocument6 paginiTimed Up and Go TestcamilaÎncă nu există evaluări
- Mkou MMDocument12 paginiMkou MMPrasetiyo WilliamÎncă nu există evaluări
- Postural Instability in Patients With Parkinson's DiseaseDocument16 paginiPostural Instability in Patients With Parkinson's Diseasemirco cortinovisÎncă nu există evaluări
- Parkinson's Disease and Parkinsonism: Review Neurology Series Editor, William J. Mullally, MDDocument6 paginiParkinson's Disease and Parkinsonism: Review Neurology Series Editor, William J. Mullally, MDBart X GankÎncă nu există evaluări
- 20 Health Benefits of CoffeeDocument4 pagini20 Health Benefits of CoffeeMunzir HassanÎncă nu există evaluări
- Resume: Om Prakash .Gaddameedi S/o SatyanarayanaDocument2 paginiResume: Om Prakash .Gaddameedi S/o SatyanarayanavaddemkiranÎncă nu există evaluări
- Group 1 Parkinsons Pre TestDocument4 paginiGroup 1 Parkinsons Pre TestAyman NabilÎncă nu există evaluări
- Combination of Honey and L-Dopa Protected The Dopaminergic Neurons Against MPTP Induced Parkinsonism in Adult Male Swiss MiceDocument6 paginiCombination of Honey and L-Dopa Protected The Dopaminergic Neurons Against MPTP Induced Parkinsonism in Adult Male Swiss MiceInternational Journal of Innovative Science and Research Technology100% (1)
- Parkinsonismo VascularDocument9 paginiParkinsonismo VascularAna María Saldaña BenavidesÎncă nu există evaluări
- Learning Plan - SafetyDocument9 paginiLearning Plan - Safetyapi-341527743Încă nu există evaluări
- ParkinsonsDocument22 paginiParkinsonsHrudhay LuckyÎncă nu există evaluări
- Introduction to Community Health and EpidemiologyDocument35 paginiIntroduction to Community Health and EpidemiologyMark Johnson Dela PeñaÎncă nu există evaluări
- Clinical Pearls in Tremor and Other Hyperkinetic MovimentDocument7 paginiClinical Pearls in Tremor and Other Hyperkinetic Movimentrafael rocha novaesÎncă nu există evaluări
- An Efficient Machine Learning Approach For Diagnosing Parkinson's Disease by Utilizing Voice FeaturesDocument20 paginiAn Efficient Machine Learning Approach For Diagnosing Parkinson's Disease by Utilizing Voice Featuresarti ranaÎncă nu există evaluări