S-ar putea să vă placă și
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Paediatric ProtocolsDocument434 paginiPaediatric ProtocolsJashveerBediÎncă nu există evaluări
- Certificate For COVID-19 Vaccination: Beneficiary DetailsDocument1 paginăCertificate For COVID-19 Vaccination: Beneficiary DetailsBɽaŋded DɘvɪlÎncă nu există evaluări
- Vicp Fact SheetDocument2 paginiVicp Fact SheetDaniela OpreaÎncă nu există evaluări
- Pediatrics Slides 23C 2020 8 Banvir 1aDocument344 paginiPediatrics Slides 23C 2020 8 Banvir 1aBanvir SinghÎncă nu există evaluări
- CertificateDocument1 paginăCertificateAmit Kumar SenÎncă nu există evaluări
- Baby Immunization ScheduleDocument1 paginăBaby Immunization Schedulesunil kalaÎncă nu există evaluări
- Bin NgadiluwihDocument24 paginiBin NgadiluwihDeni HasanÎncă nu există evaluări
- Seir Linelist TemplateDocument16 paginiSeir Linelist TemplateCharlotte Luntok LeonÎncă nu există evaluări
- Name of Doctors AddressDocument18 paginiName of Doctors AddressSita Ram ChaudharyÎncă nu există evaluări
- Clinic - Rules - Extension 2Document12 paginiClinic - Rules - Extension 2Tony LeMesmerÎncă nu există evaluări
- Pediatric DermatologyDocument5 paginiPediatric DermatologyHina AbbasÎncă nu există evaluări
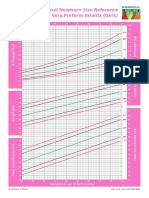
- Intergrowth21 Newborn Size Reference Charts (Girls)Document2 paginiIntergrowth21 Newborn Size Reference Charts (Girls)Anonymous MWd5UOUuiyÎncă nu există evaluări
- Changing Trends in Pediatrics and Pediatric NursingDocument18 paginiChanging Trends in Pediatrics and Pediatric NursingSakshi AsthanaÎncă nu există evaluări
- SBI Deped Batangas 8 8 19Document38 paginiSBI Deped Batangas 8 8 19Lee-Ann ZerimarÎncă nu există evaluări
- ParticipantCaseWorksheets 072018Document11 paginiParticipantCaseWorksheets 072018Saul0% (7)
- TetanusDocument2 paginiTetanusmegreen GamingÎncă nu există evaluări
- Breast FeedingDocument2 paginiBreast FeedingBRYANNMÎncă nu există evaluări
- Doh Ro Xi Pms Form No. 6Document4 paginiDoh Ro Xi Pms Form No. 6Kheanne Loise San LuisÎncă nu există evaluări
- Neonatal Jaundice PathwayDocument35 paginiNeonatal Jaundice PathwayMcmac YangoÎncă nu există evaluări
- Medical Services - Alphabetical List (A-Z), Best Healthcare, Latest Medical Technology - UCLA Health, Los Angeles, CADocument8 paginiMedical Services - Alphabetical List (A-Z), Best Healthcare, Latest Medical Technology - UCLA Health, Los Angeles, CAsunny siligamÎncă nu există evaluări
- Epi PediaDocument1 paginăEpi Pediag3nj1Încă nu există evaluări
- High School TranscriptsDocument3 paginiHigh School Transcriptsapi-485483448Încă nu există evaluări
- PTDF 5Document27 paginiPTDF 5mofiyinfolu100% (2)
- Pediatric Cardiac AnamnesisDocument3 paginiPediatric Cardiac Anamnesissofia butron friasÎncă nu există evaluări
- 496Document1 pagină496Suman MondalÎncă nu există evaluări
- College Annual Report 2003-2004Document41 paginiCollege Annual Report 2003-2004stevetkwongÎncă nu există evaluări
- Questions About Children's Flu VaccinationDocument2 paginiQuestions About Children's Flu VaccinationANNAÎncă nu există evaluări
- SOP Penanganan Pertusis (Whooping Cough)Document4 paginiSOP Penanganan Pertusis (Whooping Cough)puskesmas padang100% (1)
- Govt Scheme Economics (Sanket Sir)Document32 paginiGovt Scheme Economics (Sanket Sir)Suraj WadbudeÎncă nu există evaluări
- Tika Utsav Vaccination Sites (21.06.2021) : SR No Uphc/Phc Actual Site Name VaccineDocument3 paginiTika Utsav Vaccination Sites (21.06.2021) : SR No Uphc/Phc Actual Site Name VaccineKayÎncă nu există evaluări