S-ar putea să vă placă și
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (74)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- Philippine Education Deteriorating - EditedDocument3 paginiPhilippine Education Deteriorating - EditedRukimi Yamato100% (1)
- The One With The ThumbDocument4 paginiThe One With The Thumbnoelia20_09Încă nu există evaluări
- PathologyDocument31 paginiPathologyStudy Usmle100% (1)
- EP07 Measuring Coefficient of Viscosity of Castor OilDocument2 paginiEP07 Measuring Coefficient of Viscosity of Castor OilKw ChanÎncă nu există evaluări
- An Enhanced Radio Network Planning Methodology For GSM-R CommunicationsDocument4 paginiAn Enhanced Radio Network Planning Methodology For GSM-R CommunicationsNuno CotaÎncă nu există evaluări
- Dynamic Study of Parabolic Cylindrical Shell A Parametric StudyDocument4 paginiDynamic Study of Parabolic Cylindrical Shell A Parametric StudyEditor IJTSRDÎncă nu există evaluări
- Ode To The West WindDocument4 paginiOde To The West WindCharis Mae DimaculanganÎncă nu există evaluări
- Ty Baf TaxationDocument4 paginiTy Baf TaxationAkki GalaÎncă nu există evaluări
- Retail Branding and Store Loyalty - Analysis in The Context of Reciprocity, Store Accessibility, and Retail Formats (PDFDrive)Document197 paginiRetail Branding and Store Loyalty - Analysis in The Context of Reciprocity, Store Accessibility, and Retail Formats (PDFDrive)Refu Se ShitÎncă nu există evaluări
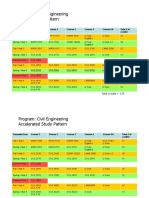
- HKUST 4Y Curriculum Diagram CIVLDocument4 paginiHKUST 4Y Curriculum Diagram CIVLfrevÎncă nu există evaluări
- Tenses English Grammar PresentationDocument14 paginiTenses English Grammar PresentationMaz Gedi60% (5)
- SHS G11 Reading and Writing Q3 Week 1 2 V1Document15 paginiSHS G11 Reading and Writing Q3 Week 1 2 V1Romeo Espinosa Carmona JrÎncă nu există evaluări
- MEMORANDUM OF AGREEMENT DraftsDocument3 paginiMEMORANDUM OF AGREEMENT DraftsRichard Colunga80% (5)
- HangersSupportsReferenceDataGuide PDFDocument57 paginiHangersSupportsReferenceDataGuide PDFIndra RosadiÎncă nu există evaluări
- Communicating Value - PatamilkaDocument12 paginiCommunicating Value - PatamilkaNeha ArumallaÎncă nu există evaluări
- Tec066 6700 PDFDocument2 paginiTec066 6700 PDFExclusivo VIPÎncă nu există evaluări
- Exclusive GA MCQs For IBPS Clerk MainDocument136 paginiExclusive GA MCQs For IBPS Clerk MainAnkit MauryaÎncă nu există evaluări
- Saudi Methanol Company (Ar-Razi) : Job Safety AnalysisDocument7 paginiSaudi Methanol Company (Ar-Razi) : Job Safety AnalysisAnonymous voA5Tb0Încă nu există evaluări
- Eje Delantero Fxl14 (1) .6Document2 paginiEje Delantero Fxl14 (1) .6Lenny VirgoÎncă nu există evaluări
- Financial Institutions Markets and ServicesDocument2 paginiFinancial Institutions Markets and ServicesPavneet Kaur Bhatia100% (1)
- Sheetal PatilDocument4 paginiSheetal PatilsheetalÎncă nu există evaluări
- CHN Nutri LabDocument4 paginiCHN Nutri LabMushy_ayaÎncă nu există evaluări
- 5045.CHUYÊN ĐỀDocument8 pagini5045.CHUYÊN ĐỀThanh HuyềnÎncă nu există evaluări
- GrenTech Express Communication System Introduction 1.0Document30 paginiGrenTech Express Communication System Introduction 1.0Son NguyenÎncă nu există evaluări
- Less Homework More TroubleDocument7 paginiLess Homework More Troubleg697a0mw100% (1)
- Chapter1 Intro To Basic FinanceDocument28 paginiChapter1 Intro To Basic FinanceRazel GopezÎncă nu există evaluări
- Outlook of PonDocument12 paginiOutlook of Ponty nguyenÎncă nu există evaluări
- SL Generator Ultrasunete RincoDocument2 paginiSL Generator Ultrasunete RincoDariaÎncă nu există evaluări
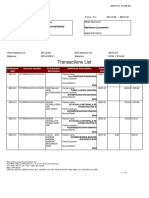
- Transactions List: Marilena Constantin RO75BRDE445SV93146784450 RON Marilena ConstantinDocument12 paginiTransactions List: Marilena Constantin RO75BRDE445SV93146784450 RON Marilena ConstantinConstantin MarilenaÎncă nu există evaluări
- BSNL BillDocument3 paginiBSNL BillKaushik GurunathanÎncă nu există evaluări