S-ar putea să vă placă și
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- National Income: Where It Comes From and Where It Goes: MacroeconomicsDocument36 paginiNational Income: Where It Comes From and Where It Goes: MacroeconomicsSarah SeunarineÎncă nu există evaluări
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- Econ 2000 Tutorial Sheet 1Document6 paginiEcon 2000 Tutorial Sheet 1Sarah SeunarineÎncă nu există evaluări
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- Science Tech UndergradDocument5 paginiScience Tech UndergradSarah SeunarineÎncă nu există evaluări
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (399)
- Algebra SG Notes V 3.3 PDFDocument82 paginiAlgebra SG Notes V 3.3 PDFSarah SeunarineÎncă nu există evaluări
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- The Science of Macroeconomics: AcroeconomicsDocument29 paginiThe Science of Macroeconomics: AcroeconomicsDeri YantoÎncă nu există evaluări
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Consumption: MACROECONOMICS, 7th. Edition N. Gregory Mankiw Mannig J. Simidian, Modified by MebDocument56 paginiConsumption: MACROECONOMICS, 7th. Edition N. Gregory Mankiw Mannig J. Simidian, Modified by MebSarah SeunarineÎncă nu există evaluări
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Science Tech UndergradDocument5 paginiScience Tech UndergradSarah SeunarineÎncă nu există evaluări
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Science Department UWIDocument190 paginiScience Department UWIZamCreativeÎncă nu există evaluări
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- Caribbean Studies Internal AssessmentDocument30 paginiCaribbean Studies Internal AssessmentSarah SeunarineÎncă nu există evaluări
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Back Cover 1Document1 paginăBack Cover 1Sarah SeunarineÎncă nu există evaluări
- Caribbean Studies Internal AssessmentDocument37 paginiCaribbean Studies Internal AssessmentSarah SeunarineÎncă nu există evaluări
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- Caribbean Studies Internal AssessmentDocument31 paginiCaribbean Studies Internal AssessmentSarah SeunarineÎncă nu există evaluări
- Caribbean Studies Internal AssessmentDocument30 paginiCaribbean Studies Internal AssessmentSarah SeunarineÎncă nu există evaluări
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- Comment SheetDocument1 paginăComment SheetSarah SeunarineÎncă nu există evaluări
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (73)
- Drug Trafficking InfoDocument5 paginiDrug Trafficking InfoSarah SeunarineÎncă nu există evaluări
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- Book Cover 1Document1 paginăBook Cover 1Sarah SeunarineÎncă nu există evaluări
- COMP 1602 Summer TimetableDocument1 paginăCOMP 1602 Summer TimetableSarah SeunarineÎncă nu există evaluări
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- COMP 1602 Summer TimetableDocument1 paginăCOMP 1602 Summer TimetableSarah SeunarineÎncă nu există evaluări
- 5.1 Review of For LoopsDocument14 pagini5.1 Review of For LoopsSarah SeunarineÎncă nu există evaluări
- Probability Theory II Summer TimetableDocument1 paginăProbability Theory II Summer TimetableSarah SeunarineÎncă nu există evaluări
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- Drug Trafficking and The Community PDFDocument4 paginiDrug Trafficking and The Community PDFSarah SeunarineÎncă nu există evaluări
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- Drug Trafficking and The Community PDFDocument4 paginiDrug Trafficking and The Community PDFSarah SeunarineÎncă nu există evaluări
- Drug Trafficking InfoDocument5 paginiDrug Trafficking InfoSarah SeunarineÎncă nu există evaluări
- Science Department UWIDocument190 paginiScience Department UWIZamCreativeÎncă nu există evaluări
- Sequential Statements and Variables: HelloworldDocument10 paginiSequential Statements and Variables: HelloworldSarah SeunarineÎncă nu există evaluări
- Repetition With While Loops: 10.1 Sequence, Selection, and RepetitionDocument12 paginiRepetition With While Loops: 10.1 Sequence, Selection, and RepetitionSarah SeunarineÎncă nu există evaluări
- Files: Hello, How Are You?Document16 paginiFiles: Hello, How Are You?Sarah SeunarineÎncă nu există evaluări
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Selecting Alternatives With If-Then-Else Statements: Remainder Num % 2Document17 paginiSelecting Alternatives With If-Then-Else Statements: Remainder Num % 2Sarah SeunarineÎncă nu există evaluări
- Flow Charts and Repetition Statements: For LoopDocument11 paginiFlow Charts and Repetition Statements: For LoopSarah SeunarineÎncă nu există evaluări
- Barack ObamaDocument3 paginiBarack ObamaVijay KumarÎncă nu există evaluări
- Phase DiagramDocument3 paginiPhase DiagramTing TCÎncă nu există evaluări
- N6867e PXLP 3000Document7 paginiN6867e PXLP 3000talaporriÎncă nu există evaluări
- Eurocode Conference 2023 Seters Van Eurocode 7Document33 paginiEurocode Conference 2023 Seters Van Eurocode 7Rodolfo BlanchiettiÎncă nu există evaluări
- Aspen Plus User ModelsDocument339 paginiAspen Plus User Modelskiny81100% (1)
- ADAMS/View Function Builder: Run-Time FunctionsDocument185 paginiADAMS/View Function Builder: Run-Time FunctionsSrinivasarao YenigallaÎncă nu există evaluări
- Excavation Trench Permit Ex 1 F0206Document5 paginiExcavation Trench Permit Ex 1 F0206emeka2012Încă nu există evaluări
- EE 8602 - Protection and Switchgear Unit I - MCQ BankDocument11 paginiEE 8602 - Protection and Switchgear Unit I - MCQ Bankpoonam yadavÎncă nu există evaluări
- Ahmed Amr P2Document8 paginiAhmed Amr P2Ahmed AmrÎncă nu există evaluări
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- FmatterDocument12 paginiFmatterNabilAlshawish0% (2)
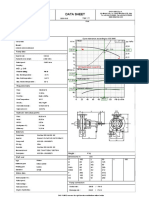
- Data Sheet: Item N°: Curve Tolerance According To ISO 9906Document3 paginiData Sheet: Item N°: Curve Tolerance According To ISO 9906Aan AndianaÎncă nu există evaluări
- Sim Educ101Document101 paginiSim Educ101Rolando AmadÎncă nu există evaluări
- Focal Length of Convex LensDocument5 paginiFocal Length of Convex LensHey AnuragÎncă nu există evaluări
- Design of CouplingDocument75 paginiDesign of CouplingVatsal BhalaniÎncă nu există evaluări
- The Genius of Marie Curie Shohini GhoseDocument4 paginiThe Genius of Marie Curie Shohini GhoseMarta HrynyovskaÎncă nu există evaluări
- DC Motor: F Bli NewtonDocument35 paginiDC Motor: F Bli NewtonMuhammad TausiqueÎncă nu există evaluări
- Curriculum Improvement v2Document47 paginiCurriculum Improvement v2Nica Lagrimas100% (1)
- Exp - P7 - UPCTDocument11 paginiExp - P7 - UPCTSiddesh PatilÎncă nu există evaluări
- SR# Call Type A-Party B-Party Date & Time Duration Cell ID ImeiDocument12 paginiSR# Call Type A-Party B-Party Date & Time Duration Cell ID ImeiSaifullah BalochÎncă nu există evaluări
- Electric PotentialDocument26 paginiElectric PotentialGlitchÎncă nu există evaluări
- Efektifitas Terapi Musik Klasik Terhadap Penurunan Tingkat HalusinasiDocument9 paginiEfektifitas Terapi Musik Klasik Terhadap Penurunan Tingkat HalusinasiAnis RahmaÎncă nu există evaluări
- TOPIC: Movable and Immovable Property Under Section-3 of Transfer of Property ActDocument10 paginiTOPIC: Movable and Immovable Property Under Section-3 of Transfer of Property ActRishAbh DaidÎncă nu există evaluări
- Jarir IT Flyer Qatar1Document4 paginiJarir IT Flyer Qatar1sebincherianÎncă nu există evaluări
- Lalkitab Varshphal Chart PDFDocument6 paginiLalkitab Varshphal Chart PDFcalvinklein_22ukÎncă nu există evaluări
- PLASSON UK July 2022 Price Catalogue v1Document74 paginiPLASSON UK July 2022 Price Catalogue v1Jonathan Ninapaytan SanchezÎncă nu există evaluări
- EE360 - Magnetic CircuitsDocument48 paginiEE360 - Magnetic Circuitsبدون اسمÎncă nu există evaluări
- Vectors Notes (Answers)Document24 paginiVectors Notes (Answers)ScionÎncă nu există evaluări
- High Performance Vector Control SE2 Series InverterDocument9 paginiHigh Performance Vector Control SE2 Series InverterhanazahrÎncă nu există evaluări
- Manual - Rapid Literacy AssessmentDocument16 paginiManual - Rapid Literacy AssessmentBaldeo PreciousÎncă nu există evaluări
- Abstract Cohort 1 Clin Psych FZ 20220323Document31 paginiAbstract Cohort 1 Clin Psych FZ 20220323Azizah OthmanÎncă nu există evaluări
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedDe la EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedEvaluare: 5 din 5 stele5/5 (80)
- The Obesity Code: Unlocking the Secrets of Weight LossDe la EverandThe Obesity Code: Unlocking the Secrets of Weight LossEvaluare: 4 din 5 stele4/5 (6)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDDe la EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDEvaluare: 5 din 5 stele5/5 (1)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeDe la EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeEvaluare: 2 din 5 stele2/5 (1)
- The Age of Magical Overthinking: Notes on Modern IrrationalityDe la EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityEvaluare: 4 din 5 stele4/5 (24)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionDe la EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionEvaluare: 4 din 5 stele4/5 (404)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisDe la EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisEvaluare: 4.5 din 5 stele4.5/5 (42)