S-ar putea să vă placă și
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- Diabetes in TeensDocument5 paginiDiabetes in TeensAlmas PrawotoÎncă nu există evaluări
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Condiloma AkuminataDocument3 paginiCondiloma AkuminataAlmas PrawotoÎncă nu există evaluări
- Journal Reading IKK ANHDocument15 paginiJournal Reading IKK ANHAlmas PrawotoÎncă nu există evaluări
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- Pengelolaan Kasus: Cutaneous Changes in Venous and Lymphatic InsufficiencyDocument4 paginiPengelolaan Kasus: Cutaneous Changes in Venous and Lymphatic InsufficiencyAlmas PrawotoÎncă nu există evaluări
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- Hawaii Hotel NumberDocument1 paginăHawaii Hotel NumberAlmas PrawotoÎncă nu există evaluări
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- Identifying Risk For Diabetes in Adolescence (Irda) : A Pilot Study in General PracticeDocument12 paginiIdentifying Risk For Diabetes in Adolescence (Irda) : A Pilot Study in General PracticeAlmas PrawotoÎncă nu există evaluări
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (399)
- Side Effects of NSAIDsDocument8 paginiSide Effects of NSAIDsAlmas PrawotoÎncă nu există evaluări
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- Why Is Long-Term Therapy Required To Cure Tuberculosis?: Research in TranslationDocument8 paginiWhy Is Long-Term Therapy Required To Cure Tuberculosis?: Research in TranslationMonica Herdiati Rukmana NaibahoÎncă nu există evaluări
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- Bab 1Document2 paginiBab 1Almas PrawotoÎncă nu există evaluări
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- Perioperative Planning & Pain ManagementDocument18 paginiPerioperative Planning & Pain ManagementAlmas PrawotoÎncă nu există evaluări
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Oxford Perioperative Pain Management 2013Document141 paginiOxford Perioperative Pain Management 2013Almas PrawotoÎncă nu există evaluări
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Damage ControlDocument8 paginiDamage ControlAlmas PrawotoÎncă nu există evaluări
- Hawaii Travel PlanDocument103 paginiHawaii Travel PlanAlmas PrawotoÎncă nu există evaluări
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (73)
- Hidronefrosis PDFDocument54 paginiHidronefrosis PDFAlmas PrawotoÎncă nu există evaluări
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- OsteomyelitisDocument5 paginiOsteomyelitisAlmas PrawotoÎncă nu există evaluări
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- Guideline PresbycusisDocument4 paginiGuideline PresbycusisAlmas PrawotoÎncă nu există evaluări
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- Journal Ischemic StrokeDocument9 paginiJournal Ischemic StrokeAlmas PrawotoÎncă nu există evaluări
- Interpretasi RontgenDocument12 paginiInterpretasi RontgenAlmas PrawotoÎncă nu există evaluări
- Official Reprint From Uptodate ©2017 UptodateDocument9 paginiOfficial Reprint From Uptodate ©2017 UptodateAlmas Prawoto100% (1)
- Official Reprint From Uptodate ©2017 UptodateDocument9 paginiOfficial Reprint From Uptodate ©2017 UptodateAlmas Prawoto100% (1)
- Fracture ManagementDocument4 paginiFracture ManagementAlmas PrawotoÎncă nu există evaluări
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- Meniscus Injury: Almas PrawotoDocument9 paginiMeniscus Injury: Almas PrawotoAlmas PrawotoÎncă nu există evaluări
- Fracture ManagementDocument4 paginiFracture ManagementAlmas PrawotoÎncă nu există evaluări
- Anterior Cruciate Ligament InjuriesDocument16 paginiAnterior Cruciate Ligament InjuriesAlmas PrawotoÎncă nu există evaluări
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- Post TraumaDocument5 paginiPost TraumaAlmas PrawotoÎncă nu există evaluări
- The Case For Increased Research On Male FertilityDocument23 paginiThe Case For Increased Research On Male FertilityIndyra AlencarÎncă nu există evaluări
- B5 Lecture Slides (CMF) Folate AntagonistsDocument15 paginiB5 Lecture Slides (CMF) Folate AntagonistsZhen Yuan GaryÎncă nu există evaluări
- Leprosy: Pathogenesis Updated: ReviewDocument15 paginiLeprosy: Pathogenesis Updated: ReviewagneselimÎncă nu există evaluări
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (120)
- Dentin Dysplasia Type1 - Clinical ManagemenDocument3 paginiDentin Dysplasia Type1 - Clinical Managemenluncat2anÎncă nu există evaluări
- Private TutorialDocument6 paginiPrivate TutorialHoàngQuýPhiÎncă nu există evaluări
- Special Access List of Covid-19 Test Kit (For Professional Use Only)Document2 paginiSpecial Access List of Covid-19 Test Kit (For Professional Use Only)Devina FernsÎncă nu există evaluări
- Biology SL P2Document8 paginiBiology SL P2KenanÎncă nu există evaluări
- This Study Resource Was Shared Via: My CoursesDocument7 paginiThis Study Resource Was Shared Via: My CoursesRcel Balmes100% (1)
- Tau-Targeting Antisense Oligonucleotide Mapt in Mild Alzheimer's Disease: A Phase 1b, Randomized, Placebo-Controlled TrialDocument20 paginiTau-Targeting Antisense Oligonucleotide Mapt in Mild Alzheimer's Disease: A Phase 1b, Randomized, Placebo-Controlled TrialSiddharth NarsipurÎncă nu există evaluări
- Icsa Usmle Courses ContentDocument18 paginiIcsa Usmle Courses ContentdostoviskyÎncă nu există evaluări
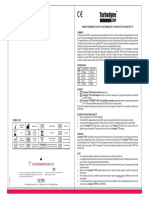
- Turbodyne: Tulip Diagnostics (P) LTDDocument2 paginiTurbodyne: Tulip Diagnostics (P) LTDMatibar RahmanÎncă nu există evaluări
- Cytogenetics, FISH and Molecular Testing in Hematologic Malignancies, 2008, p.334 PDFDocument334 paginiCytogenetics, FISH and Molecular Testing in Hematologic Malignancies, 2008, p.334 PDFJorge Santos100% (1)
- Lab Report 1: Dna Extraction From Peripheral Blood Mononuclear Cells (PBMC)Document7 paginiLab Report 1: Dna Extraction From Peripheral Blood Mononuclear Cells (PBMC)Nida RidzuanÎncă nu există evaluări
- High Risk PregnancyDocument8 paginiHigh Risk PregnancyIbrahim AdnanÎncă nu există evaluări
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
- ASDA Packet I-K (Part 1)Document48 paginiASDA Packet I-K (Part 1)Kelly KouchÎncă nu există evaluări
- Molecular Cell Biology Practice QuestionsDocument9 paginiMolecular Cell Biology Practice Questionssahana2791100% (1)
- Full Paper AIC 2018Document28 paginiFull Paper AIC 2018yantiÎncă nu există evaluări
- Understanding The Basics of DNA Fingerprinting in Forensic ScienceDocument4 paginiUnderstanding The Basics of DNA Fingerprinting in Forensic SciencevivekÎncă nu există evaluări
- Abbot, Diabetes ManagementDocument1 paginăAbbot, Diabetes ManagementMelissa Grace DizonÎncă nu există evaluări
- Chronic Wasting DiseaseDocument8 paginiChronic Wasting DiseaseNydiaCastilloÎncă nu există evaluări
- Tura KuDocument104 paginiTura KuFitzgerald BillyÎncă nu există evaluări
- Biology Paper 1 MsDocument20 paginiBiology Paper 1 Mssohaib0% (1)
- Pregnancy Induced HypertensionDocument4 paginiPregnancy Induced HypertensionclubsanatateÎncă nu există evaluări
- CytogeneticsDocument5 paginiCytogeneticsDennyvie Ann D. CeñidozaÎncă nu există evaluări
- Science Form 4 (Monthly Test)Document3 paginiScience Form 4 (Monthly Test)ma'ein100% (1)
- Genetic EngineeringDocument14 paginiGenetic Engineering4L Anisha SieudassÎncă nu există evaluări
- The Nervous System PDFDocument3 paginiThe Nervous System PDFPerry SinÎncă nu există evaluări
- Embriologi 1Document15 paginiEmbriologi 1Suhail UmarÎncă nu există evaluări
- 2019 32 Notifn Vet Asst SurgDocument26 pagini2019 32 Notifn Vet Asst SurgThiru NavukarasuÎncă nu există evaluări
- Post Traumatic Stress Disorder Research Fact SheetDocument5 paginiPost Traumatic Stress Disorder Research Fact SheetSofia MarcelinoÎncă nu există evaluări
- The Obesity Code: Unlocking the Secrets of Weight LossDe la EverandThe Obesity Code: Unlocking the Secrets of Weight LossEvaluare: 4 din 5 stele4/5 (6)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsDe la EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsÎncă nu există evaluări
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeDe la EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeEvaluare: 2 din 5 stele2/5 (1)
- The Age of Magical Overthinking: Notes on Modern IrrationalityDe la EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityEvaluare: 4 din 5 stele4/5 (24)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaDe la EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaEvaluare: 4.5 din 5 stele4.5/5 (266)