S-ar putea să vă placă și
- Central Line Cheat SheetDocument1 paginăCentral Line Cheat SheetLara Mae100% (1)
- Medical Prioritization ProcessDocument20 paginiMedical Prioritization ProcessIGDÎncă nu există evaluări
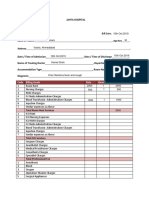
- Final - HOSPITAL BILL FORMAT PDFDocument2 paginiFinal - HOSPITAL BILL FORMAT PDFH C83% (12)
- Community Leader Awards 2010Document39 paginiCommunity Leader Awards 2010Surrey/North Delta LeaderÎncă nu există evaluări
- Streamline Healthcare ClaimsDocument2 paginiStreamline Healthcare ClaimsMJVP0% (1)
- Philippine Health Care During ErapDocument9 paginiPhilippine Health Care During ErapCristine Dela Cruz0% (2)
- NATIONAL CONSORTIUM FOR Ph.D. IN NURSING: EFFECTIVENESS OF EMOTIONAL INTELLIGENCE SKILL TRAININGDocument3 paginiNATIONAL CONSORTIUM FOR Ph.D. IN NURSING: EFFECTIVENESS OF EMOTIONAL INTELLIGENCE SKILL TRAININGRio RioÎncă nu există evaluări
- HydrocephalusDocument9 paginiHydrocephalusDeby AnditaÎncă nu există evaluări
- The "Weekend Effect" in Pediatric Surgery - Increased Mortality.2014Document5 paginiThe "Weekend Effect" in Pediatric Surgery - Increased Mortality.2014Valmir MouraÎncă nu există evaluări
- Polan Er 2012Document12 paginiPolan Er 2012nurfitriaÎncă nu există evaluări
- Fatal and Near-Fatal Asthma in Children: The Critical Care PerspectiveDocument11 paginiFatal and Near-Fatal Asthma in Children: The Critical Care PerspectiveElvis Rodríguez PalmaÎncă nu există evaluări
- 0126 Kochanek11Document7 pagini0126 Kochanek11FaisallrizzaÎncă nu există evaluări
- Patient Safety During Sedation by Anesthesia ProfeDocument8 paginiPatient Safety During Sedation by Anesthesia ProfeIsmar MorenoÎncă nu există evaluări
- Elkhunovich2016 The Utility of Cranial Ultrasound For Detection of IntracranialDocument6 paginiElkhunovich2016 The Utility of Cranial Ultrasound For Detection of IntracranialModou NianeÎncă nu există evaluări
- Regional Anesthesia in Pediatric Orthopedics A CL 2022Document9 paginiRegional Anesthesia in Pediatric Orthopedics A CL 2022Alejandra SanchezÎncă nu există evaluări
- Expert Consensus Statement Management of Pediatric Persistent ObstructiveDocument16 paginiExpert Consensus Statement Management of Pediatric Persistent ObstructiveThomasMáximoMancinelliRinaldoÎncă nu există evaluări
- The Pediatric Sedation Unit: A Mechanism For Pediatric SedationDocument9 paginiThe Pediatric Sedation Unit: A Mechanism For Pediatric SedationSantosa TandiÎncă nu există evaluări
- Early Mobilization in The Pediatric Intensive Care Unit A Systematic ReviewDocument6 paginiEarly Mobilization in The Pediatric Intensive Care Unit A Systematic ReviewJuly ZaballaÎncă nu există evaluări
- Age-Dependent Outcomes in Asymptomatic Umbilical Hernia RepairDocument6 paginiAge-Dependent Outcomes in Asymptomatic Umbilical Hernia RepairAnisaa GayatriÎncă nu există evaluări
- Dise Expert Consensus-Aao-2021Document14 paginiDise Expert Consensus-Aao-2021Alejandra Oliveros VargasÎncă nu există evaluări
- Impact of Staffing On Bloodstream Infections in The Neonatal Intensive Care UnitDocument5 paginiImpact of Staffing On Bloodstream Infections in The Neonatal Intensive Care Unitزينب محمد عبدÎncă nu există evaluări
- Medical Decision Making Among Adolescents With Neonatal Brachial Plexus Palsy and Their Families: A Qualitative StudyDocument8 paginiMedical Decision Making Among Adolescents With Neonatal Brachial Plexus Palsy and Their Families: A Qualitative StudyPaoloLansangÎncă nu există evaluări
- Apnea After Awake Regional and General Anesthesia in InfantsDocument17 paginiApnea After Awake Regional and General Anesthesia in InfantsmluthfidunandÎncă nu există evaluări
- Comparative Efficacy of Anti-Epileptic Drugs For Neonatal Seizures: A Network Meta - AnalysisDocument8 paginiComparative Efficacy of Anti-Epileptic Drugs For Neonatal Seizures: A Network Meta - AnalysisSultan Rahmat SeptianÎncă nu există evaluări
- The Pediatric "Floating Knee" Injury: A State-of-the-Art Multicenter StudyDocument7 paginiThe Pediatric "Floating Knee" Injury: A State-of-the-Art Multicenter StudyManiDeep ReddyÎncă nu există evaluări
- Jurnal UtamaDocument9 paginiJurnal UtamajanakaÎncă nu există evaluări
- Pediatrics 2012 Yee E298 304Document9 paginiPediatrics 2012 Yee E298 304Amber CarterÎncă nu există evaluări
- CirPed Diferença JPS 2014Document6 paginiCirPed Diferença JPS 2014Valmir MouraÎncă nu există evaluări
- [19330715 - Journal of Neurosurgery_ Pediatrics] Comparative effectiveness of flexible versus rigid neuroendoscopy for endoscopic third ventriculostomy and choroid plexus cauterization_ a propensity score–matchedDocument7 pagini[19330715 - Journal of Neurosurgery_ Pediatrics] Comparative effectiveness of flexible versus rigid neuroendoscopy for endoscopic third ventriculostomy and choroid plexus cauterization_ a propensity score–matchedBruno MañonÎncă nu există evaluări
- Assessing developmental delay in children using evidence-based approachesDocument3 paginiAssessing developmental delay in children using evidence-based approachesNovie AstiniÎncă nu există evaluări
- Improving The Identification of Neonatal Web VideoDocument3 paginiImproving The Identification of Neonatal Web VideoBelén AracelyÎncă nu există evaluări
- INFANIBDocument8 paginiINFANIBandrea sierraÎncă nu există evaluări
- Lidocaina Versus Articaina 2021Document7 paginiLidocaina Versus Articaina 2021Francisca Abarca CifuentesÎncă nu există evaluări
- Use of The Skeletal Survey in The Evaluation of Child MaltreatmentDocument3 paginiUse of The Skeletal Survey in The Evaluation of Child MaltreatmentAprilia DhammashintaÎncă nu există evaluări
- Elisson Et Al., 1985 Construction of An Infant Neurological InternationalDocument8 paginiElisson Et Al., 1985 Construction of An Infant Neurological InternationalSantiago Gonzalez ArdilaÎncă nu există evaluări
- Articol 1Document7 paginiArticol 1nistor97Încă nu există evaluări
- Saluja 2017Document6 paginiSaluja 2017AndikaÎncă nu există evaluări
- 1377 FullDocument23 pagini1377 FullPutri Wahyuni AllfazmyÎncă nu există evaluări
- VOTE PSR AnakDocument9 paginiVOTE PSR AnakINGGRID 102015016Încă nu există evaluări
- Difficult or Impossible Facemask Ventilation in Children With DifficultDocument10 paginiDifficult or Impossible Facemask Ventilation in Children With Difficultema moralesÎncă nu există evaluări
- Comparative Videolaryngoscope Performance in Children: Data From The Pediatric Difficult Intubation RegistryDocument3 paginiComparative Videolaryngoscope Performance in Children: Data From The Pediatric Difficult Intubation RegistryTan AndiÎncă nu există evaluări
- Prospectivo - Grunwell2017Document8 paginiProspectivo - Grunwell2017MecheVSÎncă nu există evaluări
- Intranasal Ketamine For Procedural Sedation and Analgesia in Children: A Systematic ReviewDocument15 paginiIntranasal Ketamine For Procedural Sedation and Analgesia in Children: A Systematic ReviewNADIA VICUÑA CRIADOÎncă nu există evaluări
- Paediatric Early Warning SysteDocument14 paginiPaediatric Early Warning SysteTengku rasyidÎncă nu există evaluări
- 1394 FullDocument9 pagini1394 FullDanielle AndreiÎncă nu există evaluări
- 2014 IIHTTDesignand MethodsDocument12 pagini2014 IIHTTDesignand MethodsSIMON PEREZ LOPEZÎncă nu există evaluări
- Group Lit Rev PaperDocument15 paginiGroup Lit Rev PaperChelsea RuthrauffÎncă nu există evaluări
- 3. khemani2009Document7 pagini3. khemani2009Dwi Putri SekariniÎncă nu există evaluări
- Epilepsy in Children With Shunted HydrocephalusDocument16 paginiEpilepsy in Children With Shunted HydrocephalusPauleen Trisha SamparaniÎncă nu există evaluări
- Skin Care For Pediatric2Document7 paginiSkin Care For Pediatric2Sri Nauli Dewi LubisÎncă nu există evaluări
- Accepted Manuscript: Pediatric NeurologyDocument31 paginiAccepted Manuscript: Pediatric NeurologyFarin MauliaÎncă nu există evaluări
- Estudio SafeDocument10 paginiEstudio SafePaloma Rojas BarretasÎncă nu există evaluări
- Original Research: Neonatal Peripherally Inserted Central Catheter Practices and ProvidersDocument13 paginiOriginal Research: Neonatal Peripherally Inserted Central Catheter Practices and ProvidersWinarti RimadhaniÎncă nu există evaluări
- Journal of Clinical Anesthesia: Original ContributionDocument6 paginiJournal of Clinical Anesthesia: Original ContributionzaimmuhtarÎncă nu există evaluări
- Preoperative Identification of Neurosurgery Patients With A High Risk of In-Hospital Complications: A Prospective Cohort of 418 Consecutive Elective Craniotomy PatientsDocument11 paginiPreoperative Identification of Neurosurgery Patients With A High Risk of In-Hospital Complications: A Prospective Cohort of 418 Consecutive Elective Craniotomy PatientsAzizi AlfyanÎncă nu există evaluări
- 1 MultimethodassessmentDocument8 pagini1 MultimethodassessmentRoberto Alexis Molina CampuzanoÎncă nu există evaluări
- Literatür 1Document6 paginiLiteratür 1Oguzhan KumÎncă nu există evaluări
- Neuromuscular Electrical Stimulation For Children With Dysphagia - A Systematic ReviewDocument11 paginiNeuromuscular Electrical Stimulation For Children With Dysphagia - A Systematic ReviewJaviera PalmaÎncă nu există evaluări
- Articulo Hernia OriginalDocument7 paginiArticulo Hernia OriginalmelvaÎncă nu există evaluări
- Integrative Review 1Document17 paginiIntegrative Review 1api-442558242Încă nu există evaluări
- Robert K. Fitzgerald - Multicenter Analysis of The Factors Associated With Unplanned Extubation in The PICUDocument7 paginiRobert K. Fitzgerald - Multicenter Analysis of The Factors Associated With Unplanned Extubation in The PICUKevin Bazán TorrealvaÎncă nu există evaluări
- A Behavioral Method For Efficient Screening of Visual Acuity in Young InfantsDocument9 paginiA Behavioral Method For Efficient Screening of Visual Acuity in Young InfantsWistya Eka mahadewiÎncă nu există evaluări
- Subconj Hemorrhage and AbuseDocument5 paginiSubconj Hemorrhage and AbuseNurul Annisa muthaharaÎncă nu există evaluări
- Jurnal 6Document17 paginiJurnal 6Dhiny RatuÎncă nu există evaluări
- Adverse Events in The Neonatal Intensive Care UnitDocument12 paginiAdverse Events in The Neonatal Intensive Care UnitevangelinasÎncă nu există evaluări
- Monitoring the Nervous System for Anesthesiologists and Other Health Care ProfessionalsDe la EverandMonitoring the Nervous System for Anesthesiologists and Other Health Care ProfessionalsÎncă nu există evaluări
- Anesthetic Management for the Pediatric Airway: Advanced Approaches and TechniquesDe la EverandAnesthetic Management for the Pediatric Airway: Advanced Approaches and TechniquesDiego PreciadoÎncă nu există evaluări
- Postoperative Cognitive Dysfunction Preoperative Risk Assessment and Perioperative Risk Minimization A Pragmatic Review of The LitDocument5 paginiPostoperative Cognitive Dysfunction Preoperative Risk Assessment and Perioperative Risk Minimization A Pragmatic Review of The Litade_liaÎncă nu există evaluări
- Remifentanil Update: Clinical Science and UtilityDocument20 paginiRemifentanil Update: Clinical Science and Utilityade_liaÎncă nu există evaluări
- Remifentanil Update: Clinical Science and UtilityDocument20 paginiRemifentanil Update: Clinical Science and Utilityade_liaÎncă nu există evaluări
- Remifentanil Compared With Midazolam and Pethidine Sedation During Colonoscopy: A Prospective, Randomized StudyDocument7 paginiRemifentanil Compared With Midazolam and Pethidine Sedation During Colonoscopy: A Prospective, Randomized Studyade_liaÎncă nu există evaluări
- Comparison of Remifentanil With Fentanyl For Deep Sedation in Oral SurgeryDocument8 paginiComparison of Remifentanil With Fentanyl For Deep Sedation in Oral Surgeryade_liaÎncă nu există evaluări
- 2016 - Observational Research Methods. Research Design II Cohort, Cross Sectional, and Case-Control StudiesDocument8 pagini2016 - Observational Research Methods. Research Design II Cohort, Cross Sectional, and Case-Control StudiesamarillonoexpectaÎncă nu există evaluări
- Kritall APRASIALDocument7 paginiKritall APRASIALHaidar ShiddiqÎncă nu există evaluări
- 1 s2.0 S0914508712003139 MainDocument6 pagini1 s2.0 S0914508712003139 Mainade_liaÎncă nu există evaluări
- Kritall APRASIALDocument7 paginiKritall APRASIALHaidar ShiddiqÎncă nu există evaluări
- Use Only: Anesthetics Considerations in PeritonitisDocument9 paginiUse Only: Anesthetics Considerations in Peritonitisade_liaÎncă nu există evaluări
- Cohort Studies: Prospective Versus Retrospective: Kidney Disease and Population HealthDocument5 paginiCohort Studies: Prospective Versus Retrospective: Kidney Disease and Population Healthade_liaÎncă nu există evaluări
- Newman 2001Document9 paginiNewman 2001ade_liaÎncă nu există evaluări
- Septic Peritonitis: CE ArticleDocument15 paginiSeptic Peritonitis: CE Articleade_liaÎncă nu există evaluări
- Intraoperative Fluid Management in Open Gastro-Intestinal Surgery: Goal-Directed Versus RestrictiveDocument7 paginiIntraoperative Fluid Management in Open Gastro-Intestinal Surgery: Goal-Directed Versus Restrictiveade_liaÎncă nu există evaluări
- The Use of Fluids in Sepsis: University of Central Florida College of MedicineDocument8 paginiThe Use of Fluids in Sepsis: University of Central Florida College of Medicineade_liaÎncă nu există evaluări
- HK MJ 165057Document10 paginiHK MJ 165057ade_liaÎncă nu există evaluări
- Effect of Intraoperative Fluid Management On Outcome After Intraabdominal SurgeryDocument8 paginiEffect of Intraoperative Fluid Management On Outcome After Intraabdominal Surgeryade_liaÎncă nu există evaluări
- Prone Position in Mechanically Ventilated Patients - The Hard or The Soft Way?Document2 paginiProne Position in Mechanically Ventilated Patients - The Hard or The Soft Way?ade_liaÎncă nu există evaluări
- Intraoperative Fluid Management in Open Gastro-Intestinal Surgery: Goal-Directed Versus RestrictiveDocument7 paginiIntraoperative Fluid Management in Open Gastro-Intestinal Surgery: Goal-Directed Versus Restrictiveade_liaÎncă nu există evaluări
- E-Resources in Health Sciences: by Sukhdev SinghDocument95 paginiE-Resources in Health Sciences: by Sukhdev Singhade_liaÎncă nu există evaluări
- Intraoperative Naloxone Reduces Remifentanil-Induced Postoperative Hyperalgesia But Not Pain: A Randomized Controlled TrialDocument8 paginiIntraoperative Naloxone Reduces Remifentanil-Induced Postoperative Hyperalgesia But Not Pain: A Randomized Controlled Trialade_liaÎncă nu există evaluări
- Journal Pone 0158137Document19 paginiJournal Pone 0158137ade_liaÎncă nu există evaluări
- Effects of Prone Position On The Oxygenation of Patients With Acute Respiratory Distress SyndromeDocument6 paginiEffects of Prone Position On The Oxygenation of Patients With Acute Respiratory Distress Syndromeade_liaÎncă nu există evaluări
- Hfov 2Document9 paginiHfov 2ade_liaÎncă nu există evaluări
- 1998 Effects of Prone On Resp Mech Gas ExchDocument7 pagini1998 Effects of Prone On Resp Mech Gas Exchade_liaÎncă nu există evaluări
- Prono y ALI 2011Document6 paginiProno y ALI 2011ade_liaÎncă nu există evaluări
- Pic C - GuerinDocument33 paginiPic C - Guerinade_liaÎncă nu există evaluări
- Ball 2001Document11 paginiBall 2001ade_liaÎncă nu există evaluări
- 1998 Effects of Prone On Resp Mech Gas ExchDocument7 pagini1998 Effects of Prone On Resp Mech Gas Exchade_liaÎncă nu există evaluări
- Courtenay Savage DissertationDocument230 paginiCourtenay Savage DissertationcesavageÎncă nu există evaluări
- PEDIATRIC PARENTERAL NUTRITIONDocument62 paginiPEDIATRIC PARENTERAL NUTRITIONPetruÎncă nu există evaluări
- Chapter 43 - Do The Surviving Sepsis Campaign Guidelines WorkDocument4 paginiChapter 43 - Do The Surviving Sepsis Campaign Guidelines WorkIkhlasul Amal WellÎncă nu există evaluări
- District Mental Health ProgramDocument6 paginiDistrict Mental Health Programaswaroop91Încă nu există evaluări
- Portfolio ReflectionDocument2 paginiPortfolio Reflectionapi-317257113Încă nu există evaluări
- Early Prediction of Severity StrokeDocument11 paginiEarly Prediction of Severity StrokeainihanifiahÎncă nu există evaluări
- Shah's Spleen 2011Document9 paginiShah's Spleen 2011gigipourÎncă nu există evaluări
- Leadership Shadowing ActivityDocument2 paginiLeadership Shadowing Activityapi-455549333Încă nu există evaluări
- Accomplishment ReportDocument8 paginiAccomplishment ReportKevin Fernandez MendioroÎncă nu există evaluări
- CCS Exam Content OutlineDocument2 paginiCCS Exam Content OutlineSundarajan ManiÎncă nu există evaluări
- JOURNAL Mam HazelDocument6 paginiJOURNAL Mam HazelBryan Voltaire Santos LannuÎncă nu există evaluări
- Vital Signs Steps: at The Same Time Check Arm Circumference To Determine Cuff Size)Document2 paginiVital Signs Steps: at The Same Time Check Arm Circumference To Determine Cuff Size)Yemaya84Încă nu există evaluări
- Local Invention During American PeriodDocument16 paginiLocal Invention During American PeriodAngelica Lyca GonzalesÎncă nu există evaluări
- List of AMP (Outdoor)Document6 paginiList of AMP (Outdoor)srk4u88Încă nu există evaluări
- ESPEN Guidelines On Nutritional Support For Polymorbid Internal Med PatDocument18 paginiESPEN Guidelines On Nutritional Support For Polymorbid Internal Med PatAmany SalamaÎncă nu există evaluări
- Critical Thinking Case Study PharmaDocument4 paginiCritical Thinking Case Study PharmaChin T. OndongÎncă nu există evaluări
- Hospital or Clinic Which Is More UsefulDocument6 paginiHospital or Clinic Which Is More UsefulAntonette RayanÎncă nu există evaluări
- Ruskin Recovering From Emergency Brain Surgery: Mentally UnstableDocument28 paginiRuskin Recovering From Emergency Brain Surgery: Mentally UnstableSan Mateo Daily JournalÎncă nu există evaluări
- Patient Hospitals Kosher Guide - Dec '09Document8 paginiPatient Hospitals Kosher Guide - Dec '09amromÎncă nu există evaluări
- Devesh CVDocument2 paginiDevesh CVanon-67433Încă nu există evaluări
- Institutionalized ChildrenDocument2 paginiInstitutionalized ChildrenMuhammad Khan KhosoÎncă nu există evaluări
- Dr. Daniel SesslerDocument2 paginiDr. Daniel SesslerKimAndersonÎncă nu există evaluări
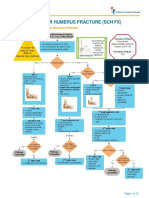
- Fracture Supracondylar HumerusDocument12 paginiFracture Supracondylar HumeruskemsÎncă nu există evaluări



























![[19330715 - Journal of Neurosurgery_ Pediatrics] Comparative effectiveness of flexible versus rigid neuroendoscopy for endoscopic third ventriculostomy and choroid plexus cauterization_ a propensity score–matched](https://imgv2-2-f.scribdassets.com/img/document/722525723/149x198/0c84be9862/1712965550?v=1)