S-ar putea să vă placă și
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDe la EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeEvaluare: 4 din 5 stele4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDe la EverandThe Little Book of Hygge: Danish Secrets to Happy LivingEvaluare: 3.5 din 5 stele3.5/5 (400)
- Preeclampsia Pathophysiology andDocument15 paginiPreeclampsia Pathophysiology andYojhaida Zarate CasachahuaÎncă nu există evaluări
- Saturacion Venosa InglesDocument7 paginiSaturacion Venosa InglesYojhaida Zarate CasachahuaÎncă nu există evaluări
- Guidelines On Perioperative Management of Anticoagulant and Antiplatelet Agents PDFDocument40 paginiGuidelines On Perioperative Management of Anticoagulant and Antiplatelet Agents PDFYojhaida Zarate CasachahuaÎncă nu există evaluări
- Management of Anaphylaxis A Systematic ReviewDocument8 paginiManagement of Anaphylaxis A Systematic ReviewYojhaida Zarate CasachahuaÎncă nu există evaluări
- 15-1010 BLS ProviderManual S PDFDocument99 pagini15-1010 BLS ProviderManual S PDFAlma Aulia100% (8)
- AnemiaDocument5 paginiAnemiaYojhaida Zarate CasachahuaÎncă nu există evaluări
- Org Ha No Phosphorus Poisoning MangementDocument11 paginiOrg Ha No Phosphorus Poisoning MangementAhmad Khalil Abou AhmadÎncă nu există evaluări
- Shoe Dog: A Memoir by the Creator of NikeDe la EverandShoe Dog: A Memoir by the Creator of NikeEvaluare: 4.5 din 5 stele4.5/5 (537)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDe la EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceEvaluare: 4 din 5 stele4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)De la EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Evaluare: 4 din 5 stele4/5 (98)
- The Emperor of All Maladies: A Biography of CancerDe la EverandThe Emperor of All Maladies: A Biography of CancerEvaluare: 4.5 din 5 stele4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDe la EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryEvaluare: 3.5 din 5 stele3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDe la EverandNever Split the Difference: Negotiating As If Your Life Depended On ItEvaluare: 4.5 din 5 stele4.5/5 (838)
- Grit: The Power of Passion and PerseveranceDe la EverandGrit: The Power of Passion and PerseveranceEvaluare: 4 din 5 stele4/5 (588)
- On Fire: The (Burning) Case for a Green New DealDe la EverandOn Fire: The (Burning) Case for a Green New DealEvaluare: 4 din 5 stele4/5 (73)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDe la EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureEvaluare: 4.5 din 5 stele4.5/5 (474)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDe la EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaEvaluare: 4.5 din 5 stele4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaDe la EverandThe Unwinding: An Inner History of the New AmericaEvaluare: 4 din 5 stele4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnDe la EverandTeam of Rivals: The Political Genius of Abraham LincolnEvaluare: 4.5 din 5 stele4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDe la EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyEvaluare: 3.5 din 5 stele3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDe la EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreEvaluare: 4 din 5 stele4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDe la EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersEvaluare: 4.5 din 5 stele4.5/5 (344)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)De la EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Evaluare: 4.5 din 5 stele4.5/5 (121)
- Her Body and Other Parties: StoriesDe la EverandHer Body and Other Parties: StoriesEvaluare: 4 din 5 stele4/5 (821)
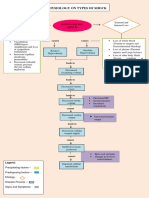
- Pathophysiology On Types of ShockDocument4 paginiPathophysiology On Types of ShockJessa Mae Alforque AsentistaÎncă nu există evaluări
- Drug StudyDocument7 paginiDrug Studykymsh_kimÎncă nu există evaluări
- Sadyapranahara Marma Shareer With Respect To TraumatologyDocument3 paginiSadyapranahara Marma Shareer With Respect To TraumatologyEditor IJTSRDÎncă nu există evaluări
- NCPDocument3 paginiNCPKrizza Ayenn MacutoÎncă nu există evaluări
- NCP For Delivery RoomDocument4 paginiNCP For Delivery RoomGiselle EstoquiaÎncă nu există evaluări
- ParacentesisDocument13 paginiParacentesisroger100% (2)
- Management Hypovolemic Shock, NurinDocument12 paginiManagement Hypovolemic Shock, Nurinرفاعي آكرمÎncă nu există evaluări
- Case Scenario: Prostate CancerDocument5 paginiCase Scenario: Prostate Cancer24 PAULINO ALDRIN MUJARÎncă nu există evaluări
- 109 Anaesthesia For The Bleeding TonsilDocument6 pagini109 Anaesthesia For The Bleeding TonsilRanjan KumarÎncă nu există evaluări
- Phtls 9th Edition Prep Packets 2019aDocument19 paginiPhtls 9th Edition Prep Packets 2019ajuan4401100% (2)
- MSF Clinical Guidelines PDFDocument356 paginiMSF Clinical Guidelines PDFKirthinath BallalÎncă nu există evaluări
- Monitoreo Hemodinamico Funcional PinskyDocument23 paginiMonitoreo Hemodinamico Funcional PinskyJuan CarrascoÎncă nu există evaluări
- 1993 92 723 Larry J. Baraff: Capillary Refill: Is It A Useful Clinical Sign?Document4 pagini1993 92 723 Larry J. Baraff: Capillary Refill: Is It A Useful Clinical Sign?Citty'Q' HuwalidÎncă nu există evaluări
- Initial Fluid Resuscitation Guided by The Parkland Formula Leads T - 2023 - BurnDocument8 paginiInitial Fluid Resuscitation Guided by The Parkland Formula Leads T - 2023 - BurnBrenda Serrano LaraÎncă nu există evaluări
- Nursing Care Plan On: "Fracture Open III A, Complete Comminuted Displaced Femur Left"Document10 paginiNursing Care Plan On: "Fracture Open III A, Complete Comminuted Displaced Femur Left"Surkhali BipanaÎncă nu există evaluări
- Treatment of Hypovolemia (Dehydration) in Children - UpToDateDocument13 paginiTreatment of Hypovolemia (Dehydration) in Children - UpToDateNedelcu MirunaÎncă nu există evaluări
- Blood Loss and Clinical SignsDocument10 paginiBlood Loss and Clinical SignsElias Emmanuel JaimeÎncă nu există evaluări
- AlbuminDocument14 paginiAlbuminMaria Chona Penillos HularÎncă nu există evaluări
- Nursing Care of Clients in Emergency Situation 2 MergedDocument234 paginiNursing Care of Clients in Emergency Situation 2 MergedDanica Franco100% (1)
- Cardiogenic ShockDocument3 paginiCardiogenic ShockDiaz AlmayangÎncă nu există evaluări
- Shock, HypovolemicDocument2 paginiShock, HypovolemicNadya Syafitri100% (2)
- Hypovolemic Shock - A Review: Drug Invention Today July 2018Document5 paginiHypovolemic Shock - A Review: Drug Invention Today July 2018AndreasÎncă nu există evaluări
- SHOCKDocument17 paginiSHOCKChithra Saju100% (1)
- Shock 1Document15 paginiShock 1kimberlygeducosornedoÎncă nu există evaluări
- Adult Nursing Skills On Complex CareDocument16 paginiAdult Nursing Skills On Complex CareNaftali OumaÎncă nu există evaluări
- Idiopathic Systemic Capillary Leak Syndrome - UpToDateDocument17 paginiIdiopathic Systemic Capillary Leak Syndrome - UpToDatenikos papamakariosÎncă nu există evaluări
- Pathophysiology of BurnsDocument7 paginiPathophysiology of BurnsTemahlungwaneÎncă nu există evaluări
- Nursing Care Plans With Nursing DiagnosisDocument6 paginiNursing Care Plans With Nursing DiagnosisLalaine RomeroÎncă nu există evaluări
- PDF NCP Fluid Volume Deficit CompressDocument2 paginiPDF NCP Fluid Volume Deficit Compressdusty kawiÎncă nu există evaluări
- Sensus Harian TGL 05 Maret 2022........Document104 paginiSensus Harian TGL 05 Maret 2022........Ruhut Putra SinuratÎncă nu există evaluări