S-ar putea să vă placă și
- Management of HyperleukocytosisDocument10 paginiManagement of HyperleukocytosisNaty AlvarezÎncă nu există evaluări
- Hyperleukocytosis, Leukostasis and Leukapheresis Practice ManagementDocument6 paginiHyperleukocytosis, Leukostasis and Leukapheresis Practice ManagementPutri Wulan Sukmawati100% (1)
- Lecture On Anemias and Polycythemias by Dr. RoomiDocument30 paginiLecture On Anemias and Polycythemias by Dr. RoomiMudassar Roomi100% (1)
- Blood Transfusion Therapy DefinitionDocument27 paginiBlood Transfusion Therapy DefinitionEvangelin MelvinÎncă nu există evaluări
- Management of Tuberculosis: A guide for clinicians (eBook edition)De la EverandManagement of Tuberculosis: A guide for clinicians (eBook edition)Încă nu există evaluări
- BMTDocument44 paginiBMTGargi MPÎncă nu există evaluări
- Blood Basics1Document6 paginiBlood Basics1Celina PastorÎncă nu există evaluări
- Kidney TransplantDocument11 paginiKidney TransplantPrincess Xzmae RamirezÎncă nu există evaluări
- Bone Marrow TransplantDocument8 paginiBone Marrow TransplantPSRI hospitalÎncă nu există evaluări
- The Benefits of Donating Blood: October 2017Document10 paginiThe Benefits of Donating Blood: October 2017MAHESH KOUJALAGIÎncă nu există evaluări
- Cerebral Venous ThrombosisDocument15 paginiCerebral Venous ThrombosisValentina RobuÎncă nu există evaluări
- Updates in Red Blood Cell and Platelet Transfusions in Preterm NeonatesDocument4 paginiUpdates in Red Blood Cell and Platelet Transfusions in Preterm NeonatesEmilio Emmanué Escobar CruzÎncă nu există evaluări
- Blood Transfusion Procedures: January 2011 Review Date: January 2013Document55 paginiBlood Transfusion Procedures: January 2011 Review Date: January 2013goldaÎncă nu există evaluări
- E Learning Geriatric Oncology An IntroductionDocument65 paginiE Learning Geriatric Oncology An IntroductionHarold JeffersonÎncă nu există evaluări
- Bone Marrow BiopsyDocument28 paginiBone Marrow BiopsyAmeer MattaÎncă nu există evaluări
- A Prospective Study of Prescribing Pattern in The Management of Stroke at A Tertiary Care HospitalDocument6 paginiA Prospective Study of Prescribing Pattern in The Management of Stroke at A Tertiary Care HospitalInternational Journal of Innovative Science and Research TechnologyÎncă nu există evaluări
- Acute Intestinal Obstruction...Document42 paginiAcute Intestinal Obstruction...Ali100% (2)
- Blood Transfusion On Dialysis Guidelines Aug 2017 PDFDocument5 paginiBlood Transfusion On Dialysis Guidelines Aug 2017 PDFYolanda IrawatiÎncă nu există evaluări
- A Study to Assess the Effectiveness of Video Assisted Teaching Module on Knowledge Regarding Myocardial Infarction and its Prevention among the Patients Attending Diabetic Clinic at BVV Sangha’s HSK Hospital and Research Centre, BagalkotDocument3 paginiA Study to Assess the Effectiveness of Video Assisted Teaching Module on Knowledge Regarding Myocardial Infarction and its Prevention among the Patients Attending Diabetic Clinic at BVV Sangha’s HSK Hospital and Research Centre, BagalkotInternational Journal of Innovative Science and Research TechnologyÎncă nu există evaluări
- BM Procedure and ProcessingDocument28 paginiBM Procedure and ProcessingNidhi JaisÎncă nu există evaluări
- Apheresis PrincipleDocument68 paginiApheresis Principlemelisa asibalÎncă nu există evaluări
- Approach To Septic ShockDocument16 paginiApproach To Septic ShockRaja EllysyaÎncă nu există evaluări
- Exchange TransfusionDocument9 paginiExchange TransfusiondewpraÎncă nu există evaluări
- Report2014 PDFDocument332 paginiReport2014 PDFShareDialysis100% (1)
- Acute Renal FailureDocument14 paginiAcute Renal FailuredrtpkÎncă nu există evaluări
- How I Use Platelet TransfusionsDocument12 paginiHow I Use Platelet TransfusionsJovanna OrtuñoÎncă nu există evaluări
- Vena Cava Superior SyndromeDocument12 paginiVena Cava Superior SyndromeAgnes SetiawanÎncă nu există evaluări
- Class Presentation ON Acute Tubular NecrosisDocument39 paginiClass Presentation ON Acute Tubular NecrosisDeeksha RajputÎncă nu există evaluări
- Seizures in Children JULIO 2020Document29 paginiSeizures in Children JULIO 2020Elizabeth HendersonÎncă nu există evaluări
- Intradialytic Stretching Exercises On Fatigueand Muscle CrampsDocument6 paginiIntradialytic Stretching Exercises On Fatigueand Muscle CrampsInternational Journal of Innovative Science and Research TechnologyÎncă nu există evaluări
- Fulminant Hepatic Failure: Nattaphol UransilpDocument27 paginiFulminant Hepatic Failure: Nattaphol UransilpChacha TasyaÎncă nu există evaluări
- 13-Cis-Retinoic Acid: It's Therapeutic Implications and Adverse EffectsDocument8 pagini13-Cis-Retinoic Acid: It's Therapeutic Implications and Adverse EffectsBoston Science Publishing100% (1)
- Coronary Artery Bypass Grafting (Cabg) :: Case Study ReportDocument83 paginiCoronary Artery Bypass Grafting (Cabg) :: Case Study ReportSherena NicolasÎncă nu există evaluări
- Bone Marrow ChecklistDocument2 paginiBone Marrow ChecklistHasyim SuparlanÎncă nu există evaluări
- Case 36 AscitesDocument4 paginiCase 36 AscitesMichaelÎncă nu există evaluări
- 3 Bone Marrow ExaminationDocument105 pagini3 Bone Marrow ExaminationShourav SarkarÎncă nu există evaluări
- Cardiac ArrestDocument10 paginiCardiac ArrestFebby Aulia AriefÎncă nu există evaluări
- Kidney TransplantDocument3 paginiKidney TransplantSuneel Kumar PrajapatiÎncă nu există evaluări
- Acute Tubular NecrosisDocument15 paginiAcute Tubular NecrosisDeepak patelÎncă nu există evaluări
- Acute Liver FailureDocument78 paginiAcute Liver FailurePankaj IngleÎncă nu există evaluări
- HRSDocument63 paginiHRSPriya KalariaÎncă nu există evaluări
- Spinal TuberculosisDocument46 paginiSpinal TuberculosisAbby Austero100% (1)
- Abdominal TuberculosisDocument28 paginiAbdominal TuberculosisNajezita Sachenka CH CÎncă nu există evaluări
- Evidence Based Medicine: What It Is and What It Isn'tDocument3 paginiEvidence Based Medicine: What It Is and What It Isn'tCristian EstradaÎncă nu există evaluări
- Critical Care Update PDFDocument25 paginiCritical Care Update PDFHugo PozoÎncă nu există evaluări
- Thrombolytic TherapyDocument37 paginiThrombolytic TherapySani sunilÎncă nu există evaluări
- Renal Transplantation: Name: Jyotishman Bharali Class: X-B Roll No: 19Document12 paginiRenal Transplantation: Name: Jyotishman Bharali Class: X-B Roll No: 19Jyotishman Bharali100% (1)
- Acute Myeloid LeukemiaDocument3 paginiAcute Myeloid LeukemiaKathleen Marie ChuangÎncă nu există evaluări
- Hepatitis GDocument8 paginiHepatitis Ghelmi0% (1)
- Problem-based Approach to Gastroenterology and HepatologyDe la EverandProblem-based Approach to Gastroenterology and HepatologyJohn N. PlevrisÎncă nu există evaluări
- Anemia and Critical CareDocument77 paginiAnemia and Critical Carehunter_axl010% (1)
- Course: Medical Surgical Nursing Ii Course Code: NSC 322 Topic: Leukamia Lecturer: Mrs Chukwu Date: Tuesday, 7Th June, 2022Document13 paginiCourse: Medical Surgical Nursing Ii Course Code: NSC 322 Topic: Leukamia Lecturer: Mrs Chukwu Date: Tuesday, 7Th June, 2022Leo D' GreatÎncă nu există evaluări
- Drug Compliance Among Hypertensive PatientsDocument5 paginiDrug Compliance Among Hypertensive PatientsSyifa MunawarahÎncă nu există evaluări
- Introduction To HematologyDocument61 paginiIntroduction To HematologyThis is PonyÎncă nu există evaluări
- Congestive Heart Failure (CHF) PDFDocument2 paginiCongestive Heart Failure (CHF) PDFZazulizer Are BackÎncă nu există evaluări
- Plasma P Here SisDocument13 paginiPlasma P Here SisSampath GoudÎncă nu există evaluări
- Infective Endocarditis: A Multidisciplinary ApproachDe la EverandInfective Endocarditis: A Multidisciplinary ApproachArman KilicÎncă nu există evaluări
- The Art of WarDocument5 paginiThe Art of WarSuwadiaya AdnyanaÎncă nu există evaluări
- Salter Bab 08 Congenital Abnormaalities PDFDocument53 paginiSalter Bab 08 Congenital Abnormaalities PDFSuwadiaya AdnyanaÎncă nu există evaluări
- WHO - Surgical Care at The District Hospital (WHO 2003)Document514 paginiWHO - Surgical Care at The District Hospital (WHO 2003)gekriaÎncă nu există evaluări
- TabelDocument1 paginăTabelSuwadiaya AdnyanaÎncă nu există evaluări
- Memory of Neonate PDFDocument7 paginiMemory of Neonate PDFSuwadiaya AdnyanaÎncă nu există evaluări
- Gender, Slum Poverty and Climate Change in Flooded River Lines in Metro ManilaDocument53 paginiGender, Slum Poverty and Climate Change in Flooded River Lines in Metro ManilaADBGADÎncă nu există evaluări
- Chewable: Buy Pepcid AC Packages, Get Pepcid AC 18'sDocument2 paginiChewable: Buy Pepcid AC Packages, Get Pepcid AC 18'sMahemoud MoustafaÎncă nu există evaluări
- Lesson 1 - Intro To Highway EngineeringDocument15 paginiLesson 1 - Intro To Highway EngineeringSaoirseÎncă nu există evaluări
- ISO - TR - 15608 - 2017 (En) - Pipe Grouping SystemsDocument12 paginiISO - TR - 15608 - 2017 (En) - Pipe Grouping SystemsTeodor ProdanÎncă nu există evaluări
- Food Processing NC II - SAGDocument4 paginiFood Processing NC II - SAGNylmazdahr Sañeud DammahomÎncă nu există evaluări
- Parche CRP 65 - Ficha Técnica - en InglesDocument2 paginiParche CRP 65 - Ficha Técnica - en IngleserwinvillarÎncă nu există evaluări
- Far Eastern University - Manila Income Taxation TAX1101 Fringe Benefit TaxDocument10 paginiFar Eastern University - Manila Income Taxation TAX1101 Fringe Benefit TaxRyan Christian BalanquitÎncă nu există evaluări
- Refinería Kirkuk PDFDocument11 paginiRefinería Kirkuk PDFcesarinarragaÎncă nu există evaluări
- Biopolymers: Overview of Several Properties and Consequences On Their ApplicationsDocument10 paginiBiopolymers: Overview of Several Properties and Consequences On Their ApplicationsrafacpereiraÎncă nu există evaluări
- Benzil PDFDocument5 paginiBenzil PDFAijaz NawazÎncă nu există evaluări
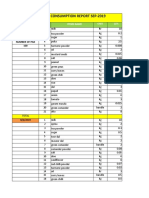
- Daily Staff Food Consumption Reports Sep-2019Document4 paginiDaily Staff Food Consumption Reports Sep-2019Manjit RawatÎncă nu există evaluări
- ResumeDocument3 paginiResumejohn DaqueÎncă nu există evaluări
- Science 9 Q4 SML17 V2Document15 paginiScience 9 Q4 SML17 V2HotdogÎncă nu există evaluări
- Electrical Data: PD2310 ApplicationsDocument1 paginăElectrical Data: PD2310 ApplicationsKSÎncă nu există evaluări
- 6 Kuliah Liver CirrhosisDocument55 pagini6 Kuliah Liver CirrhosisAnonymous vUEDx8100% (1)
- Task 5 Banksia-SD-SE-T1-Hazard-Report-Form-Template-V1.0-ID-200278Document5 paginiTask 5 Banksia-SD-SE-T1-Hazard-Report-Form-Template-V1.0-ID-200278Samir Mosquera-PalominoÎncă nu există evaluări
- Jeremy A. Greene-Prescribing by Numbers - Drugs and The Definition of Disease-The Johns Hopkins University Press (2006) PDFDocument337 paginiJeremy A. Greene-Prescribing by Numbers - Drugs and The Definition of Disease-The Johns Hopkins University Press (2006) PDFBruno de CastroÎncă nu există evaluări
- Bedwetting TCMDocument5 paginiBedwetting TCMRichonyouÎncă nu există evaluări
- GrowNote Faba South 3 Pre PlantingDocument22 paginiGrowNote Faba South 3 Pre PlantingDawitÎncă nu există evaluări
- Basics of Fire SprinklerDocument21 paginiBasics of Fire SprinklerLeo_1982Încă nu există evaluări
- Multi-Wing Engineering GuideDocument7 paginiMulti-Wing Engineering Guidea_salehiÎncă nu există evaluări
- Chapter Three Liquid Piping SystemDocument51 paginiChapter Three Liquid Piping SystemMelaku TamiratÎncă nu există evaluări
- ISO 45001:2018 & OHSAS 18001:2007 Clause-Wise Comparison MatrixDocument3 paginiISO 45001:2018 & OHSAS 18001:2007 Clause-Wise Comparison MatrixvenkatesanÎncă nu există evaluări
- How McDonald'sDocument2 paginiHow McDonald'spratik khandualÎncă nu există evaluări
- E61 DiagramDocument79 paginiE61 Diagramthanes1027Încă nu există evaluări
- Neopuff PDFDocument4 paginiNeopuff PDFoechimÎncă nu există evaluări
- Behavior Specific Praise Statements HandoutDocument3 paginiBehavior Specific Praise Statements HandoutDaniel BernalÎncă nu există evaluări
- Uas MR1Document2 paginiUas MR1IvanÎncă nu există evaluări
- Maintenance Instructions, Parts Identification & Seal Kits For Series 2H / 2HD / 2HB & 3H / 3HD / 3HBDocument10 paginiMaintenance Instructions, Parts Identification & Seal Kits For Series 2H / 2HD / 2HB & 3H / 3HD / 3HBAtaa AssaadÎncă nu există evaluări
- How To Do Banana Milk - Google Search PDFDocument1 paginăHow To Do Banana Milk - Google Search PDFyeetyourassouttamawayÎncă nu există evaluări